Myxofibrosarcoma of the scalp with difficult preoperative diagnosis:A case report and review of the literature
2020-06-17 05:54:26XiaoTingKeXiongFengYuJiYangLiuFangHuangMeiGuiChenQingQuanLai
World Journal of Clinical Cases 2020年11期
Xiao-Ting Ke, Xiong-Feng Yu, Ji-Yang Liu, Fang Huang, Mei-Gui Chen, Qing-Quan Lai
Xiao-Ting Ke, Xiong-Feng Yu, Ji-Yang Liu, Fang Huang, Mei-Gui Chen, Qing-Quan Lai,Department of CT/MRI, The Second Affiliated Hospital of Fujian Medical University,Quanzhou 362000, Fujian Province, China
Abstract
Key words: Malignant fibrous histiocytoma; Myxofibrosarcoma; Scalp; Magnetic resonance imaging; Treatment; Case report
INTRODUCTION
Myxofibrosarcoma (MFS) is a fibroblast malignant tumor with a matrix of myxoid,visible arc-like vessels, and tumor cells showing varying degrees of atypia. A MFS is the most common soft tissue sarcoma that appears in late adult life, is mainly a lowgrade malignancy, and occurs primarily in the lower extremities (77%), followed by the trunk (12%), and retroperitoneum or mediastinum (8%)[1]. Rare occurrences have been reported in the cranial cavity[2], orbit[3], maxilla[4], parotid gland[5], hypopharynx[6],sinus piriformis[7], vocal folds[8], thyroid gland[9], esophagus[10], breast[2], heart[11],aorta[2], scapular region[12], buttock[13], scrotum[14], pterygopalatine fossa[1,2], liver[2], and scalp. MSF of the scalp is extremely rare. We report a case of MFS of the scalp. A 46-year-old male with “a neoplasm in the scalp” was hospitalized and diagnosed with an MFS (highly malignant with massive necrotic lesions) by histologic evaluation and immunohistochemistry testing. A computed tomography (CT) scan and magnetic resonance imaging (MRI) indicated a mass in the scalp, but no typical "tail sign" was observed. Due to the lack of characteristic imaging features and the extremely unusual location, the diagnosis was missed. Lefkowitzet al[15]reported that the “tail sign” cannot be considered of diagnostic value for MFS as the sensitivity and specificity were approximately 80%. This case had unusual imaging findings.Moreover, the treatment for MFS is a matter of international discussion. In our case,aggressive surgery and adjuvant radiotherapy was effective. Therefore, we describe a 46-year-old male with a rare case of MFS originating from the scalp and report the unusual imaging findings to offer some reference for researchers. We discuss the MRI findings, treatment, and histologic evaluation and immunohistochemical testing in this rare case.
CASE PRESENTATION
Chief complaints
A 46-year-old male with “a neoplasm in the scalp for 6 mo” was hospitalized.
History of past illness
His medical history was unremarkable.
Personal and family histories
His family history was unremarkable.
Physical examination upon admission
On physical examination, a mass on the left forehead was palpated and measured approximately 6 cm × 3 cm. The tumor was hard without algesia or ulcerations.
Laboratory examinations
No abnormalities were found on laboratory examinations, including routine hematologic, biochemistry, and tumor markers.
Imaging examinations
A CT scan (Figure 1) showed an ovoid mass approximately 6.25 cm × 3.29 cm × 3.09 cm in the left frontal scalp with low density intermingled with equidense strips involving adjacent areas of the scalp. Contrast enhancement showed an uneven enhancement pattern. MRI (Figure 2) revealed a lesion in the left frontal region with an irregular surface, approximately 3.55 cm × 6.34 cm in size, and clear boundaries and visible separation. The adjacent skull was damaged and the dura mater was involved. The images of different sequences are as follows: T1, complex signal with dramatic low signal; T2, complex signal with dramatic high signal; T2 FLAIR, high marginal and low central signals; and DWI, high marginal and low central signals.The specimen (Figure 3) was visible to the naked eye as a mass in the scalp involving the skull and approximately 7.5 cm × 6.0 cm × 3.0 cm in size. Histologically (Figure 4),there were abundant heteromorphic spindle cells and partial nodular mucus arranged in a woven pattern with rare nuclear fission and abundant blood vessels in the interstitium. Immunohistochemical stains demonstrated the following: Vim (+); SMA(+); S-100 (-); GFAP (-); CD34 (+); and Ki-67 (+).
FINAL DIAGNOSIS
Myxofibrosarcoma of the scalp.
TREATMENT
A tumor resection (superficial) and cranioplasty were performed under general anesthesia. A horseshoe incision was made, approximately 24 cm in length, in the left frontotemporal parietal. The scalp was incised to the periosteum and the subcutaneous tumor was separated along the tumor margin. The tumor boundaries were clear and approximately 6.5 cm × 4.0 cm × 4.5 cm in size. Following surgery, the patient was returned to the ward in a stable condition. Subsequently, the patient underwent appropriate radiotherapy.
OUTCOME AND FOLLOW-UP
After surgery and subsequent radiotherapy, the patient recovered uneventfully without local recurrence or distant metastasis during a 19-mo follow-up period.
DISCUSSION
MFS is a type of malignant tumor with an unknown etiology that occurs in late adult life and mainly affects the lower and upper extremities, followed by the trunk, and retroperitoneum or mediastinum. The occurrence of head and neck MFS is rare, with a reported incidence of 2%-4%[16]. Only 21 cases of MFS in the head and neck have been reported in the literature, the clinical features of which (including our case) are summarized in Table 1.
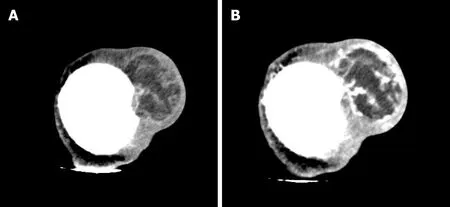
Figure 1 Computed tomography image of the patient. A: Computed tomography scan revealed that an ovoid mass with mixed density 6.25 cm × 3.29 cm × 3.09 cm in size was detected in the left frontal scalp, with low density intermingled with equidense strips involving the adjacent skull; B: Contrast enhanced computed tomography scan showed an uneven enhancement pattern.
It as shown in Table 1[17-30], there was no significant difference in the incidence of MFS in the head and neck between men and women. The age ranged from 23-87 years, and the median age was 52 years. The prognosis varied greatly depending on the time of discovery and the degree of malignancy. MFS of the scalp has not been reported; thus, the diagnosis of MFS by radiologists is difficult.
To our knowledge, a large volume, extracompartmental extension, broad interface with the underlying fascia, inhomogeneous MR signal intensity, high signal intensity on T2-weighted MR images, invasion of bone or neurovascular structures,intratumoral necrosis, and marked, primarily peripheral enhancement have been reported in the literature as malignant imaging features of soft tissue tumors[31]. The mucous component of MFS, including more water molecules, shows a higher signal at T2. The degree of high signals in T2 varies with the proportion of the mucinous component in the tumor. MRI findings of MSF contribute to establishing a diagnosis.In T2-weighted MRI, the infiltrative spread of the tumor along the fascial plane is manifested by a curvilinear shape, commonly defined as a “tail,” which extends from the primary mass of the MFS[32]; however, in several studies, MFS with a “tail-like”pattern is significantly related to a superficial (subcutaneous) origin[15]. In our case,MRI revealed a lesion with an irregular surface and a size of approximately 3.55 cm ×6.34 cm in the left frontal region, with clear boundaries and visible separation. The adjacent skull was damaged and the dura mater was involved. The MFS of the scalp of this case was a tumor of superficial (subcutaneous) origin, but the relevant MRI findings did not conform to the so-called “tail-like” pattern. Such atypical imaging findings, combined with the uncommon location, may lead radiologists to miss the correct diagnosis. Therefore, it is crucial to differentiate a MFS from other tumors with similar MRI findings, such as a low-grade fibromyxoid sarcoma (LGFS). MFS shares similar characteristics with LGFST on T1 low signals, T2 mixed signals, and an enhancing pattern; thus, the histopathologic features are required to identify a MFS[33].In addition, compared with the apparent diffusion coefficient (ADC) value of nonmyxoid tumors, that of mucinous tumors is obviously high, and DWI MR imaging has been testified as a helpful way to assess the composition of tumor cells in soft tissue sarcomas[34]. Surovet al[35]indicated that sarcomas require further study using a standardized MR program to compare the ADC values of various types of sarcomas.This idea may provide a new way for researchers to study MR of MFS in the future.
MFS can be diagnosed accurately based on immunohistologic and ultrastructural studies[16]. Histologically, myxoid cells are mixed with spindle cells. The spindle cell area is characterized by large atypical cells and more mitotic features. Mononuclear or multinucleate giant cells, curved blood vessels, spoke-like structures, and inflammatory cells are observed[32]. MFS is classified into low-grade tumors with low metastatic potential and high-grade tumors[16]. The specimen in our case was visible to the naked eye as a mass on the scalp involving the skull and approximately 7.5 cm ×6.0 cm × 3.0 cm in size. Histologically, there were abundant heteromorphic spindle cells and partial nodular mucus arranged in a woven pattern with rare nuclear fission and abundant blood vessels in the interstitium. Immunohistochemical staining demonstrated the following: Vim (+); SMA (+); S-100 (-); GFAP (-); CD34 (+); and Ki-67 (+). The histologic features combined with immunohistochemical findings in our case were consistent with mucinous fibrosarcoma (highly malignant with massive necrotic lesions). Based on the FNCLCC system, this MFS in the scalp was grade 3. In addition, the histologic findings and evaluation provided several options for the differential diagnosis, such as neurilemoma, dedifferentiated liposarcoma, and fibromatosis[16]. A MFS of grade 2-3 can be differentiated from dedifferentiated liposarcoma by immunohistochemical staining; the latter has distinctive immunohistochemical stains that are strongly positive for CKD4 and MDM2[36]. The characteristic histopathologic features of neurilemoma are the presence of abundant Wagner-Meissner corpuscle-like structures and a lack of neoplastic spindle cell nests,as seen in conventional neurofibroma and diffusely positive for S-100 by immunohistochemical analysis[37].

Figure 2 The magnetic resonance imaging revealed an irregular lesion, approximately 3.55 cm × 6.34 cm in size, in the left frontal region with clear boundaries and visible separation. The adjacent skull was damaged and the dura mater was involved. A: T1 showed complex signal with a dramatic low signal; B: T2 showed complex signal with a dramatic high signal; C: T2 FLAIR showed high marginal and low central signals; D: DWI showed high marginal and low central signals.
Based on a literature review, there has been no internationally uniform conclusion on the treatment of MFS. As far as malignant tumors are concerned, intact mass excision is advised. Additionally, the value of pre- and post-operative chemotherapy and radiotherapy is still being discussed[38]. Over the past several decades, progress in understanding sarcoma management has promoted the application of combined modality therapies to improve survival. FNCLCC grade plays a significant role in the treatment and prognosis. Therefore, the grade should be an important reference basis for clinical treatment. Some researchers have suggested that local radiotherapy of the mass for patients with FNCLCC grade 1-2 and grade 3 may be supplemented by appropriate chemotherapy and other treatments. Several studies have proposed significant reference factors for local recurrence and metastases, including tumor size,depth, extent of histologic myxoid areas, mitotic rate, and grade[15,32]. It is reported that the high rates of local recurrence of MFS are 50%-60% and distal metastases are significantly more common with high-grade MFS at a rate of 33%[16]. Given the highly malignant MFS in our case, combined with the anatomic location, size, and other factors, surgery was performed and adjuvant radiotherapy was delivered to avoid local and distant recurrences. Importantly, follow-up should be encouraged. The patient recovered without complications, without local recurrence and distant metastases after a follow-up period of 19 mo. Although there is no gold standard of treatment, a complete tumor resection with sufficient resection margins, assisted by adjuvant radiotherapy, may be effective. Dell'Aversana Orabonaet al[1]has proposed that a possible re-excision of recurrent lesions is a way to enhance survival.Additionally, the recognition of the “tail” on MRI may be valuable in pre-operative planning to ameliorate the quality of the excision, thus, reducing the risk of local recurrence[15,32]. The treatment for MSF of the scalp (highly malignant) without a “tail sign” reported in this case may provide a reference for subsequent cases that are equally atypical.

Figure 3 A mass of the scalp involving the skull approximately 7.5 cm × 6.0 cm × 3.0 cm in size.
CONCLUSION
The case reported herein of MFS occurred in an extremely rare location on the scalp and had atypical MRI findings, which serves as a reminder to radiologists of the possibility of this diagnosis to assist in clinical treatment. Although there is no gold standard of treatment, a complete tumor resection with clear resection margins,assisted by adjuvant radiotherapy, may be effective.
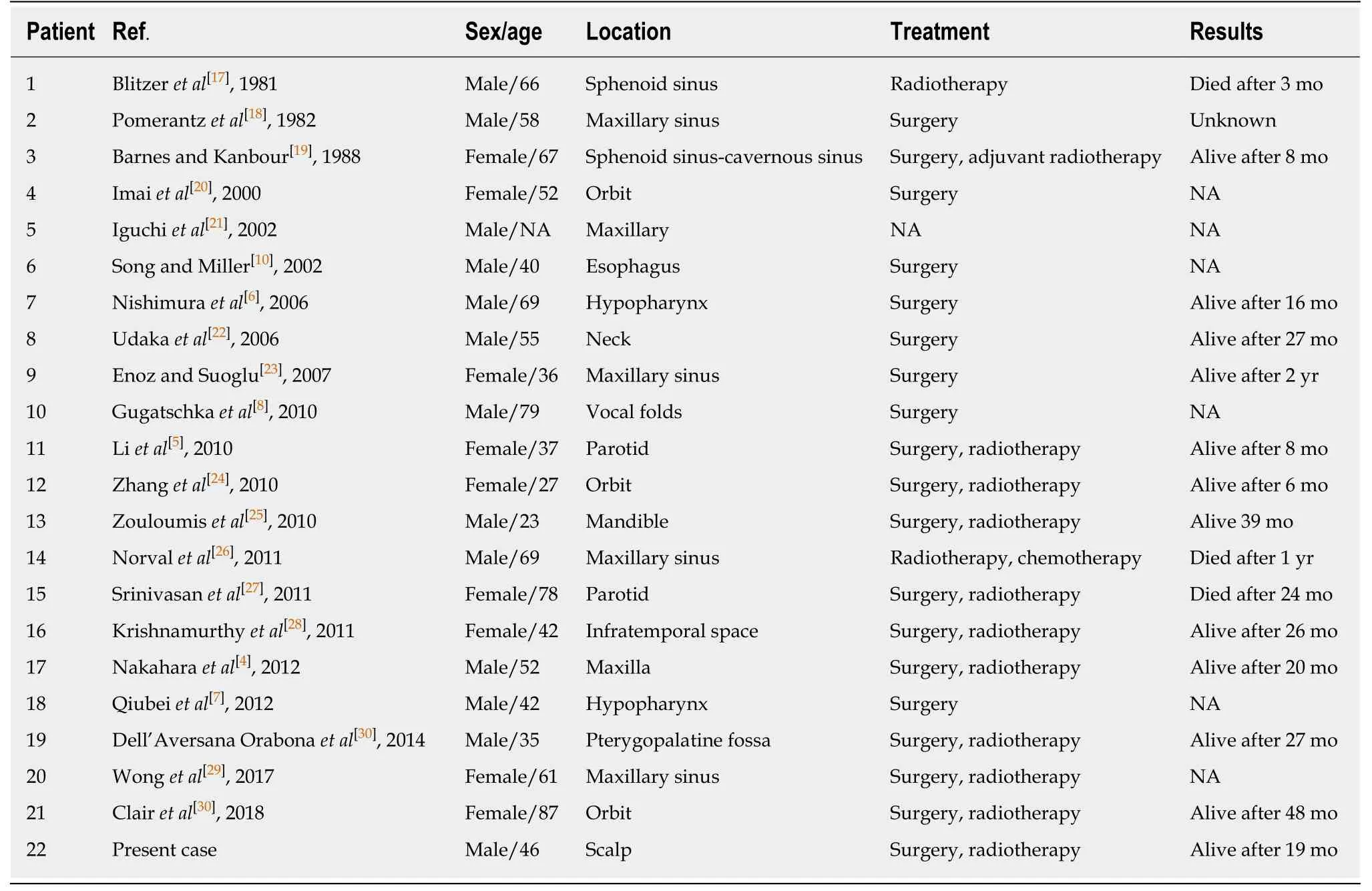
Table 1 Clinical features of head and neck myxofibrosarcoma

Figure 4 Pathologic images of the mass. Histologic evaluation showed that there were abundant heteromorphic spindle cells and partial nodular mucus, arranged in a woven pattern, with rare nuclear fission and abundant blood vessels in the interstitium (A: Hematoxylin-eosin staining, × 100, B: Hematoxylin-eosin staining, ×200).
 World Journal of Clinical Cases2020年11期
World Journal of Clinical Cases2020年11期
- World Journal of Clinical Cases的其它文章
- Macrophage activation syndrome as an initial presentation of systemic lupus erythematosus
- Optical coherence tomography guided treatment avoids stenting in an antiphospholipid syndrome patient: A case report
- Uterine incision dehiscence 3 mo after cesarean section causing massive bleeding: A case report
- Ataxia-telangiectasia complicated with Hodgkin's lymphoma: A case report
- Gastric pyloric gland adenoma resembling a submucosal tumor: A case report
- Reduced delay in diagnosis of odontogenic keratocysts with malignant transformation: A case report