A case of rhabdomyolysis with compartment syndrome in the right upper extremity
2020-05-18 01:19:28HuimingZhongGuangfengZhaoPengchaoGuo
Hui-ming Zhong, Guang-feng Zhao, Peng-chao Guo
Emergency Department, the Second Aff liated Hospital of Zhejiang University School of Medicine, Hangzhou 310009, China
Dear editor,
Acute compartment syndrome refers to a series of symptoms of muscles and nerves in the compartment of the fascia due to acute ischaemia and hypoxia. It is more common in the volar and calf of the forearm.[1]Due to long-term ischaemia of muscles and nerves in the fascia, muscle necrosis and neurological dysfunction can occur, causing serious irreversible damage to the limbs. However, rhabdomyolysis is one of the major complications in the absence of fractures or other trauma. Rhabdomyolysis syndrome refers to the destruction and disintegration of striated muscle caused by various causes, by which intracellular components such as creatine kinase and myoglobin enter the blood circulation, causing systemic disorders in the body and even acute renal failure and other clinical syndromes.[2]This case introduces rhabdomyolysis induced by skeletal muscle ischaemia and hypoxia caused by upper limb compression after drinking, accompanied by upper limb compartment syndrome.
CASE
The patient, a 31-year-old male, was admitted to the emergency department of our hospital. He complained of dizziness after drinking 2 kg of white wine 20 hours prior, and his right forearm was compressed in the prone position. When he awakened, he found himself swelling and pain in his right upper limb with numbness, limited movement of his right wrist and fi ngers, and compression of his right forearm. The patient had no recent trauma, strenuous exercise, illegal drug use, or history of other infectious diseases. He was physically healthy, with no history of hypertension, heart disease or diabetes. At the time of admission, the patient was in a good spirits, exhibited facial pain, and produced a small amount of urine with a brown colour. Physical examination showed that the right upper limb was swollen and tender, the right upper limb was tense, the right radial artery was accessible, the skin temperature of the right forearm and upper arm was fair, and the feeling was weakened. Finger movements were restricted, and the right five fi ngers all felt abnormal and showed no obvious signs of trauma. The right forearm was extended straight, the elbow was fl exed (Figure 1), tension blisters appeared, and the pain was unbearable when the fi ngers were passively extended.
Preoperative examination: creatine kinase 66,549 U/L↑, alanine aminotransferase 185 U/L↑, aspartate aminotransferase 676 U/L↑, lactate dehydrogenase 2,293 U/L↑, urinary occult blood 3+(OVER) mg/L ↑, urinary ketone body 2+ (4) mmol/L ↑, and urinary erythrocytes 56/μL ↑. Renal function and electrolytes, ECG and chest X-ray showed no abnormalities. The preliminary diagnosis was rhabdomyolysis syndrome and right upper limb osteofascial compartment syndrome. He was immediately sent to the operating room for emergency surgery.
Surgical procedure. After being anaesthetized, the patient was placed in the supine position, and his right upper extremity was routinely disinfected with a drape. An S-shaped longitudinal incision was made on the right upper extremity (Figure 1), and the skin, subcutaneous tissue, and fascia were sequentially cut. Upon exposure, the musculus biceps brachii was dark red, and there was no obvious contraction upon electrical stimulation. Incision and decompression of the medial elbow joint and decompression of the brachial artery, brachial vein and median nerve were performed. A distal incision was made to the carpal canal, the deep fascia was cut longitudinally, and the fl exor carpi ulnaris and musculus fl exor digitorum superfi cialis were separated and pulled to the sides. The ulnar artery, ulnar vein, and ulnar nerve on the surface of the flexor digitorum profundus were exposed and decompressed. The muscles of the medial forearm muscle group were bright red and contracted normally upon electrical stimulation. After relieving the pressure in the entire fascial chamber, the skin incision was not sutured. After re-irrigating the surgical area, VSD was applied under negative pressure for pressure and dressing of the wound.

Figure 1. The surgical incision during the fi rst operation.
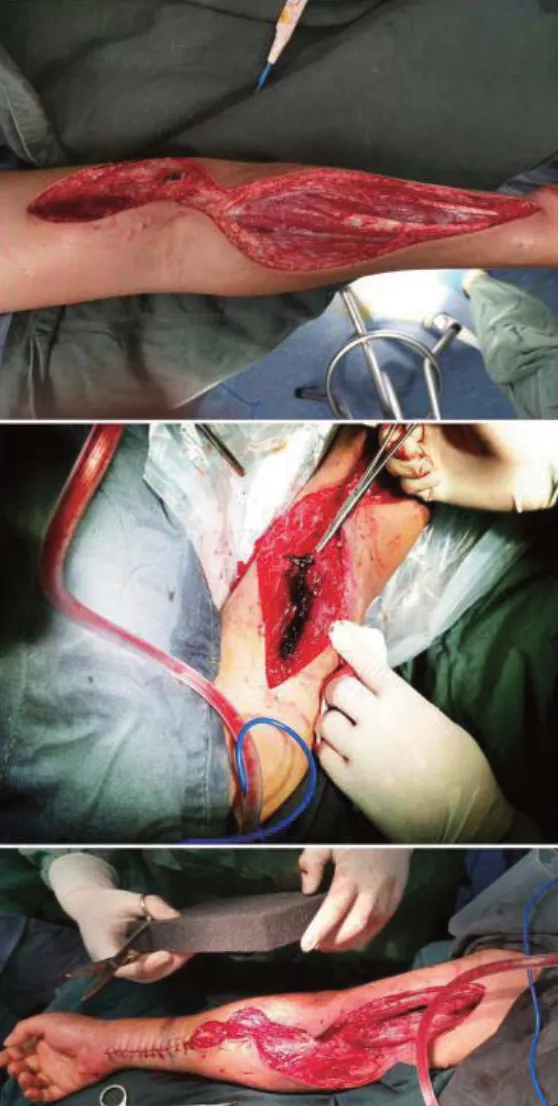
Figure 2. The necrotic tissue removed and the incision of the distal forearm sutured.
Seven days after admission, right upper extremity debridement + VSD negative pressure suction was reperformed. During the operation, the proximal biceps muscle appeared black and red, and the necrotic tissue was removed (Figure 2). The pressure of the distal forearm osteofascial compartment was significantly reduced, and debrided wound was sutured. The elbow joint and proximal upper arm fascial compartment pressure and tension were still high. After redebridement with VSD negative pressure suction, we checked that the blood flow and blood supply of the distal limb were normal. During the postoperative monitoring of creatine kinase, the key test indicators gradually decreased. The right upper limb incision was debrided and sutured 42 days after surgery, and the patient was discharged.
DISCUSSION
Osteofascial compartment syndrome (OCS) refers to a series of symptoms and signs precipitated by limb trauma caused by various reasons, leading to intracompartmental pressure (ICP) and blocking the tissue microcirculation in the osteofascial compartment.[3]Pearse et al[4]reported OCS most often occurs after trauma to the extremities, especially with long bone fractures, and the most common areas are the forearm and crus. Rhabdomyolysis syndrome is a clinical synthesis characterized by myoglobinuria, electrolyte abnormalities, and acute kidney injury resulting from the release of intracellular substances into the circulatory system due to skeletal muscle injury.[5]Clinical reports of rhabdomyolysis syndrome are not uncommon, but there are not many patients with osteofascial compartment syndrome.
In this case, the patient had right upper limb osteofascial compartment syndrome due to compression of the right upper limb for twenty hours.[6]The classic 5p symptoms are pain out of proportion, pallor, paresthesias, paralysis, and pulselessness.[7]If 3 of the clinical signs and symptoms are present, then there reportedly is a greater than 90% probability that a compartment syndrome is present.[8]The clinical manifestations of this patient were decreased urine output, brown urine, blood urea nitrogen>14.3 mmol/L, and a 100-fold increase in creatine kinase. The diagnosis and prognosis of rhabdomyolysis syndrome are related to this condition.[9]A study found that serum CK, CKMB and LDH levels in patients with suspected OCS after trauma peaked at 24 hours after injury.[10]We understood the change in the patient's condition by recording the numerical dynamic change curve of the patient.
Drug therapy for OCS is mainly used for patients with mild symptoms and early treatment, which can significantly improve the symptoms of some patients.[11]The treatment of rhabdomyolysis syndrome mainly prevents further skeletal muscle damage, prevents acute renal failure, and prevents and treats potentially life-threatening hyperkalaemia.[12]If the pain of the affected limb is aggravated, the distal limb has no arterial pulsation and the skin temperature drops; the decompression should be cut off in time to prevent the occurrence of ischaemic necrosis of the distal limb and irreversible damage.[13]After obtaining informed consent from the patient and his family, the function of the affected limb was preserved to the maximum extent. The patient's surgical method was to cut the skin and fascia, and the incision was not sutured. The wound was treated with VSD (Figure 2). The negative pressure closed drainage technique maintains the drainage negative pressure at 40-60 kPa after surgery and replaces and removes VSD after 7-10 days.[14]Functional exercises such as forearm exercises,[15]upper limb pendulum movements, internal and external shoulder joint rotation exercises, and upper arm wall climbing training were performed as early as possible after the operation.
CONCLUSION
For patients with limb crush injury and limb hypertonia, the classic 5p symptoms are helpful for osteofascial compartment syndrome diagnosis. The diagnosis of rhabdomyolysis syndrome is based on blood test results, such as elevated creatine kinase and lactic dehydrogenase. Once the condition is confirmed, incision and decompression surgery should be performed immediately. Here, the patient's wound was treated with VSD after surgery. This method can achieve decompression, improve blood circulation, rapidly promote edema regression, yield a relatively more sterilized wound surface, create conditions for the early second suture wound, and optimize time.
Funding:None.
Ethical approval:This study protocol was approved by the Ethics Committee of the hospital.
Conf icts of interest:They have no confl icts of interest.
Contributors:PCG drafted the manuscript. All authors read and approved the fi nal manuscript.
 World journal of emergency medicine2020年3期
World journal of emergency medicine2020年3期
- World journal of emergency medicine的其它文章
- Information for Readers
- Myalgia may not be associated with severity of coronavirus disease 2019 (COVID-19)
- Do PaCO2 and peripheral venous PCO2 become comparable when the peripheral venous oxygen saturation is above a certain critical value?
- Syncope in a 3-year-old male: A case report
- A case of diffuse alveolar hemorrhage following synthetic cathinone inhalation
- Evaluation of gastric lavage eff ciency and utility using a rapid quantitative method in a swine paraquat poisoning model