Scaphoid metastasis as the first sign of occult gastroesophageal junction cancer:A case report
2020-04-23 06:04:10YuJieZhangYanYanWangQiYangJianBingLi
World Journal of Clinical Cases 2020年7期
Yu-Jie Zhang,Yan-Yan Wang,Qi Yang,Jian-Bing Li
Yu-Jie Zhang,Jian-Bing Li,Department of Orthopedic Surgery,The Second Affiliated Hospital,Zhejiang University School of Medicine,Hangzhou 310009,Zhejiang Province,China
Yan-Yan Wang,Department of Oncology Surgery,The Second Affiliated Hospital,Zhejiang University School of Medicine,Hangzhou 310009,Zhejiang Province,China
Qi Yang,Department of Pathology,The Second Affiliated Hospital,Zhejiang University School of Medicine,Hangzhou 310009,Zhejiang Province,China
Abstract
Key words: Hand metastasis;Scaphoid;Gastroesophageal junction cancer;Diagnosis;Case report
INTRODUCTION
Metastases to the hand bones are rarely encountered in clinical practice and comprise approximately 0.1% of all osseous metastases[1].They can be misdiagnosed as rheumatic or infectious diseases due to the lack of specific symptoms.Usually,they are late manifestations of various advanced malignancies;however,in 16% of the affected patients,they are the initial manifestation of an occult cancer[2].Here,we report an extremely rare case of a scaphoid bone lesion that was found to be a metastasis from a gastroesophageal junction (GEJ) adenocarcinoma.
CASE PRESENTATION
Chief complaint
A 57-year-old male patient presented with persistent left wrist pain and swelling 2 mo after trauma.
History of present illness
Two months prior to this visit,the patient presented with ongoing left wrist pain and swelling after trauma.Based on an initial computed tomography (CT) scan,the patient was diagnosed with an infection of the scaphoid bone and treated with antibiotics,anti-inflammatory drugs,and rest at a local hospital.However,the pain continued to worsen,and the motion of the wrist was restricted.
History of past illness
The patient had undergone acupotomology therapy several months before the onset of the disease.He had a history of cerebral infarction and intestinal polyps.
Personal and family history
The patient was a regular drinker and heavy cigarette smoker with no relevant family history.
Physical examination upon admission
Physical examination showed left wrist tenderness,swelling,and restriction of motion with regard to radial and ulnar deviation.The swollen area was neither warm nor erythematous.
Laboratory examinations
The C-reactive protein level (49 mg/L) and the erythrocyte sedimentation rate (33 mm/h) were elevated,and the levels of tumor markers,such as carbohydrate antigen(CA)-125 (390 U/mL),carcinoembryonic antigen (CEA) (8 ng/mL),and CA211 (5.4 ng/mL),were significantly elevated.
Imaging examinations
Plain radiographs showed scaphoid bone density reduction and fracture (Figure 1A).CT and magnetic resonance imaging (MRI) scans revealed scaphoid and triangular bone destruction and soft tissue swelling,indicating a pathological fracture (Figure 1B and C).A subsequent chest CT scan suggested a lower esophageal and stomachus cardiacus mass,a right lung mass,and the destruction of multiple ribs (Figure 2A and B).We then performed positron emission tomography-CT with 2-18F fluoro-2 deoxy-D-glucose that led to a strong suspicion of GEJ and/or right lung malignancies with metastases in multiple locations,including the left lung,lymph nodes,ribs,and scapula (Figure 3).A subsequent gastroscopy did not show any space-occupying lesions (Figure 4),and the biopsy showed only chronic superficial gastritis.A CTguided percutaneous lung puncture biopsy was refused by the patient.Pathology of the left wrist showed scaphoid bone metastasis of poorly differentiated adenocarcinoma.Immunohistochemistry showed that the sample was positive for caudal type homeobox 2 (CDX2) and negative for thyroid transcription factor 1 (TTF-1) and ALK-Lung (Figure 5A).
FINAL DIAGNOSIS
The patient was diagnosed with GEJ cancer with multiple metastases.
TREATMENT
To relieve wrist pain and obtain a definite pathology,the patient underwent left scaphoid lesion resection (Figure 5B).Based on the pathology results,he was treated with two courses of chemotherapy (paclitaxel and cisplatin).He subsequently discontinued chemotherapy due to intolerance.
OUTCOME AND FOLLOW-UP
The patient died of severe interstitial pneumonia 6 mo after his initial presentation.
DISCUSSION
Bone metastases are very common in various carcinomas and mainly occur in the axial skeleton,such as the spine,pelvis,and ribs.Metastatic involvement of the hand is extremely rare.Kerin[1]demonstrated that the incidence of hand metastasis is 0.1%among all skeletal metastases.Hematogenous spread is the most common route of tumor metastasis.The hand bones have less red bone marrow,and the remoteness of the anatomical location may account for the low incidence of this disease[3].Trauma can contribute to acrometastasis.Repeated trauma may induce the production of chemotactic factors,such as prostaglandins,which promote cell migration and attachment.Additionally,the injury repair process creates an appropriate environment for tumor growth,invasion,and metastatic potential[4].The incidence of hand metastasis is higher in males than in females.The lungs,gastrointestinal tract,kidneys,and breasts are the most common primary tumor sites.Within the hand,the distal phalanges are the most frequently involved bones,followed by the metacarpals,proximal phalanges,middle phalanges,and,rarely,the carpal bones[5].To the best of our knowledge,metastasis to the carpal scaphoid bone,as was observed in our patient,has rarely been reported[6],especially as the initial symptom of a primary tumor.
The signs and symptoms of hand metastases include pain,tenderness,enlarged digits,palpable masses,ulcerations,mechanical dysfunctions,and pathological fractures,which lack specificity.Consequently,hand metastases are often misdiagnosed as osteomyelitis,soft tissue infections,gout,tenosynovitis,arthritis,or other inflammatory processes[7].Our patient was initially misdiagnosed with a bone infection.Hence,despite its rarity,orthopedic surgeons should consider the possibility of metastases to the hand bone when patients complain of persistent and progressive pain in the hand.Radiographic investigations,such as plain radiography,CT,or MRI,play vital roles in the diagnosis of hand metastases.A positron emission tomography-CT scan can help reveal the primary tumor earlier than other techniques,as it has a sensitivity greater than 90% and a specificity of 78%[8].The above imaging examinations can be used for auxiliary diagnosis;however,the final diagnosis should depend on pathology.
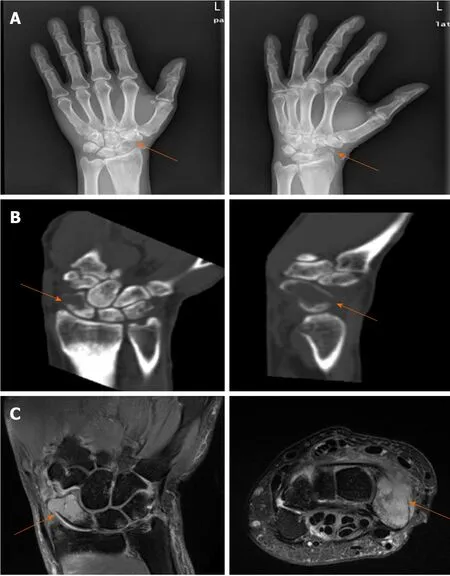
Figure1 lmaging findings in the left hand.
To date,there is no standard treatment for hand metastases[9,10].Most treatments are intended to alleviate pain and protect hand function.Radiotherapy,amputation,chemotherapy,curettage,cementation,and wide excision are the most commonly used forms of treatment.Hand metastasis often reflects the widespread dissemination of the tumor,which indicates a poor prognosis.The prognosis depends on the aggressiveness of the primary tumor.The median survival is only approximately 6 mo[1,11].
In our case,we resected the lesion to relieve the patient's discomfort and obtain pathological specimens.The pathology indicated scaphoid bone metastasis of poorly differentiated adenocarcinoma,with the characteristics of CDX2 (+),TTF-1 (-),and ALK-Lung (-).CDX2 is a pathological marker of gastrointestinal adenocarcinoma,and TTF-1 and ALK-Lung indicate lung metastatic tumors[12,13].The exophytic growth pattern of the digestive tract tumor observed on the CT scan might explain the negative results on endoscopy and biopsy.Hence,according to the clinical and pathological findings,we concluded that the scaphoid metastasis originated from a cancer of the GEJ.The GEJ is defined as the junction between the esophagus and the stomach.In this location,esophageal squamous epithelial cells gradually transition to gastric gland cells,which can be easily damaged by gastric acid reflux and are associated with a higher risk of cancer transformation[14].The incidence of GEJ adenocarcinoma has gradually increased over the last 20 years and is associated with obesity,smoking,and gastroesophageal reflux[15-18].Dysphagia and retrosternal pain are often the initial manifestations.The majority of GEJ cancer patients are initially diagnosed at an advanced stage and have a poor prognosis[19].In addition to the common sites of esophageal cancer metastases,such as the lymph nodes,lungs,liver,and bones,unexpected metastases have been increasingly reported,especially from lower esophageal cancer.The head and neck,thorax,abdominopelvic region,extremities,and multiple skin and muscle sites are the five main unexpected metastatic sites[20].Multidisciplinary management,including surgery,chemoradiotherapy,and targeted therapy,is advised[21].Surgery is the only curative treatment,while auxiliary perioperative chemoradiotherapy and targeted therapy can improve the survival rate[22,23].In this case,the patient had an advanced stage of disease and was not a candidate for surgical treatment.Immunohistochemistry showed negativity for human epidermal growth factor receptor 2;hence,trastuzumab was not used.
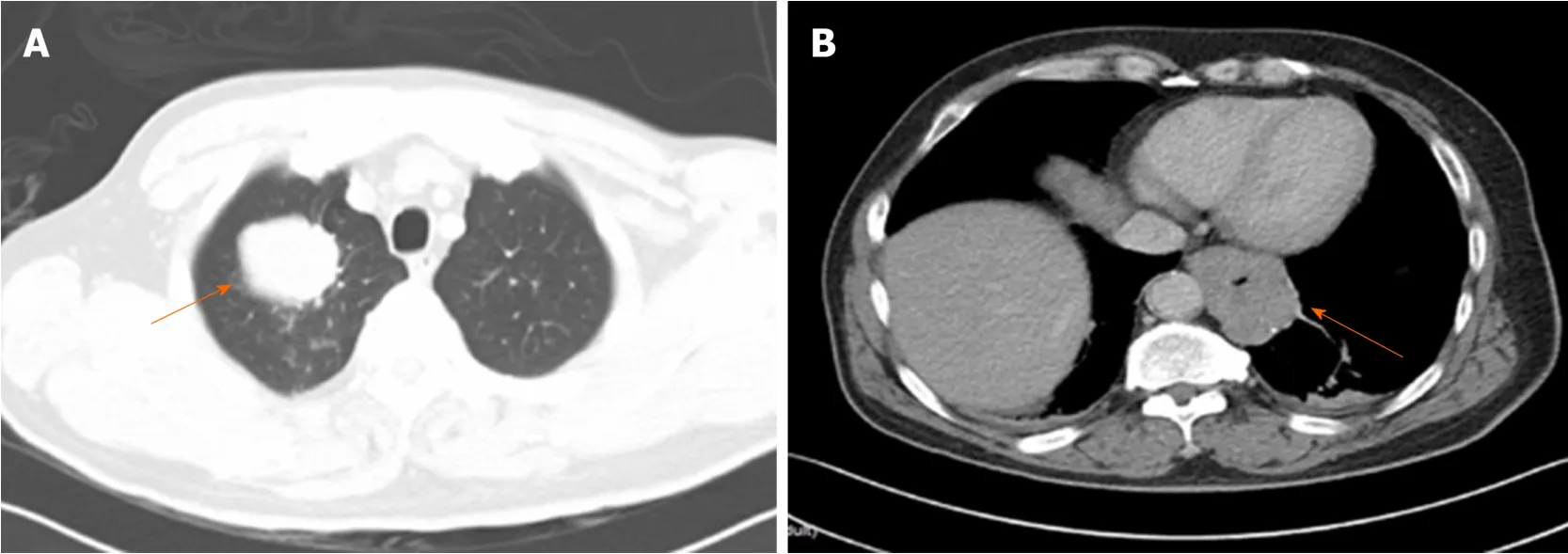
Figure2 Preoperative chest computed tomography.
In addition,because lung specimens were not available,it was difficult to determine whether the right lung mass was a secondary (metastasis) or primary tumor.After surgery,the patient's quality of life was greatly improved.However,the patient survived for only 6 mo after his initial presentation,potentially due to the delayed diagnosis and the aggressiveness of the primary tumor.Therefore,early diagnosis of metastasis to the hand bone could be helpful in that it allows the initiation of an appropriate course of treatment and prolongs survival time.
CONCLUSION
Hand metastases from solid tumors are clinically rare.Usually,they are late manifestations of advanced malignancies;however,sometimes they can be the initial manifestation of an occult cancer.Because of their low incidence and nonspecific symptoms,hand metastases are often misdiagnosed.Orthopedic surgeons should not ignore the possibility of hand metastases when patients complain of persistent and progressive pain in the hand.The treatment of hand metastasis is individualized and based on the clinical symptoms and characteristics of the primary tumor.The prognosis is generally poor.It is therefore important for clinicians to detect and diagnose these cancers early.
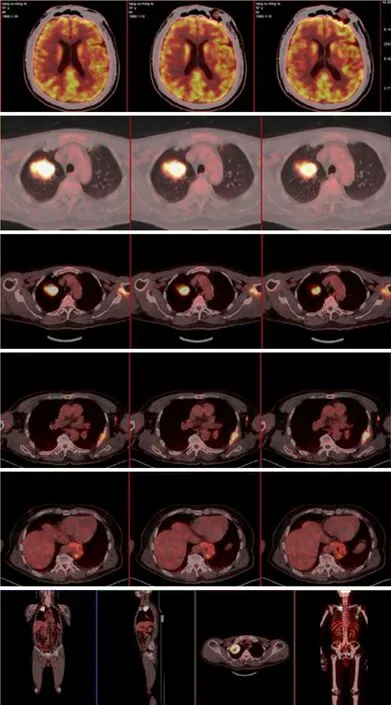
Figure3 A preoperative 2-18F fluoro-2 deoxy-D-glucose positron emission tomography-computed tomography scan showed multiple malignant lesions throughout the whole body.
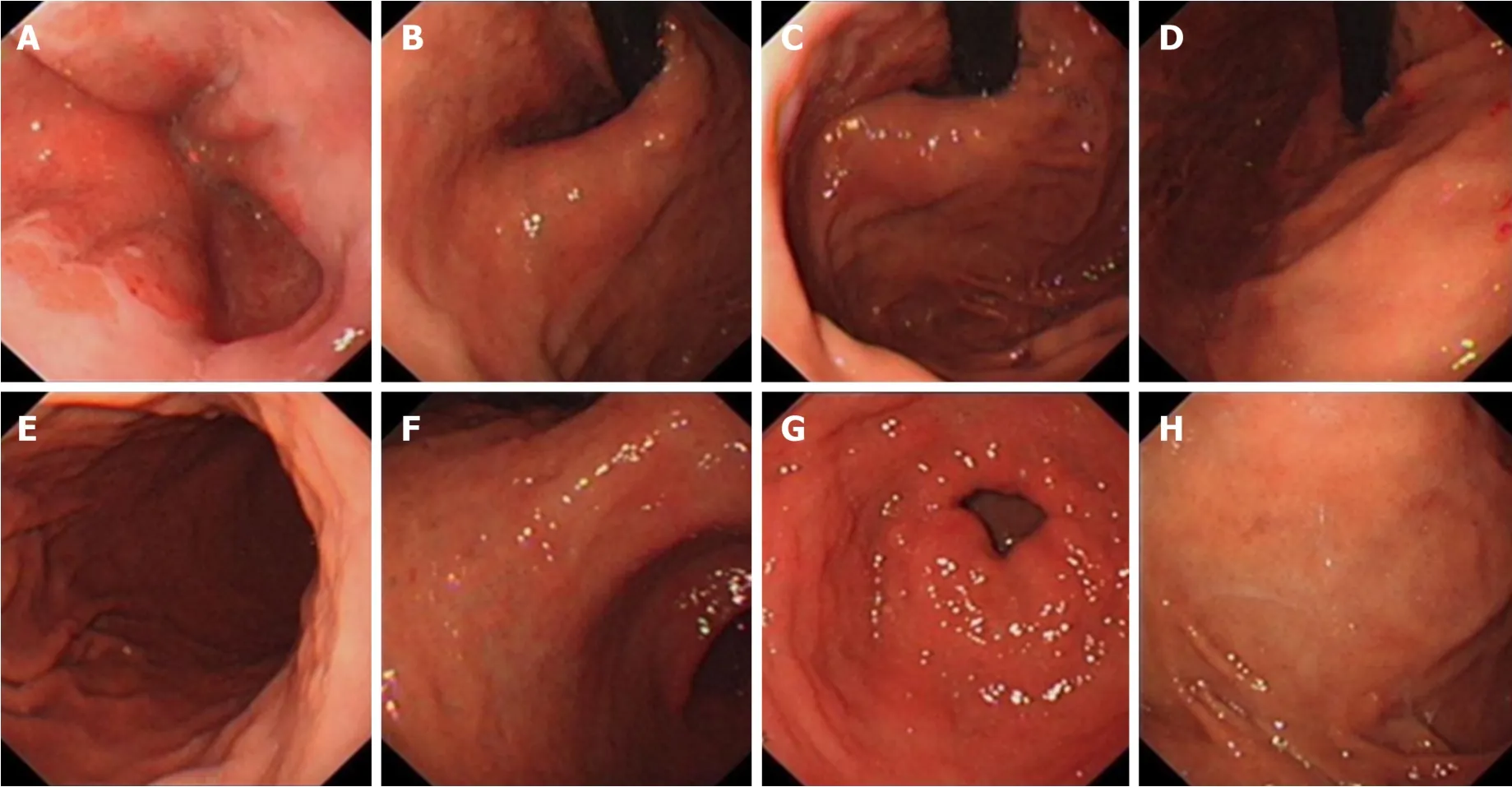
Figure4 Preoperative gastroscopy did not find any space-occupying lesions.
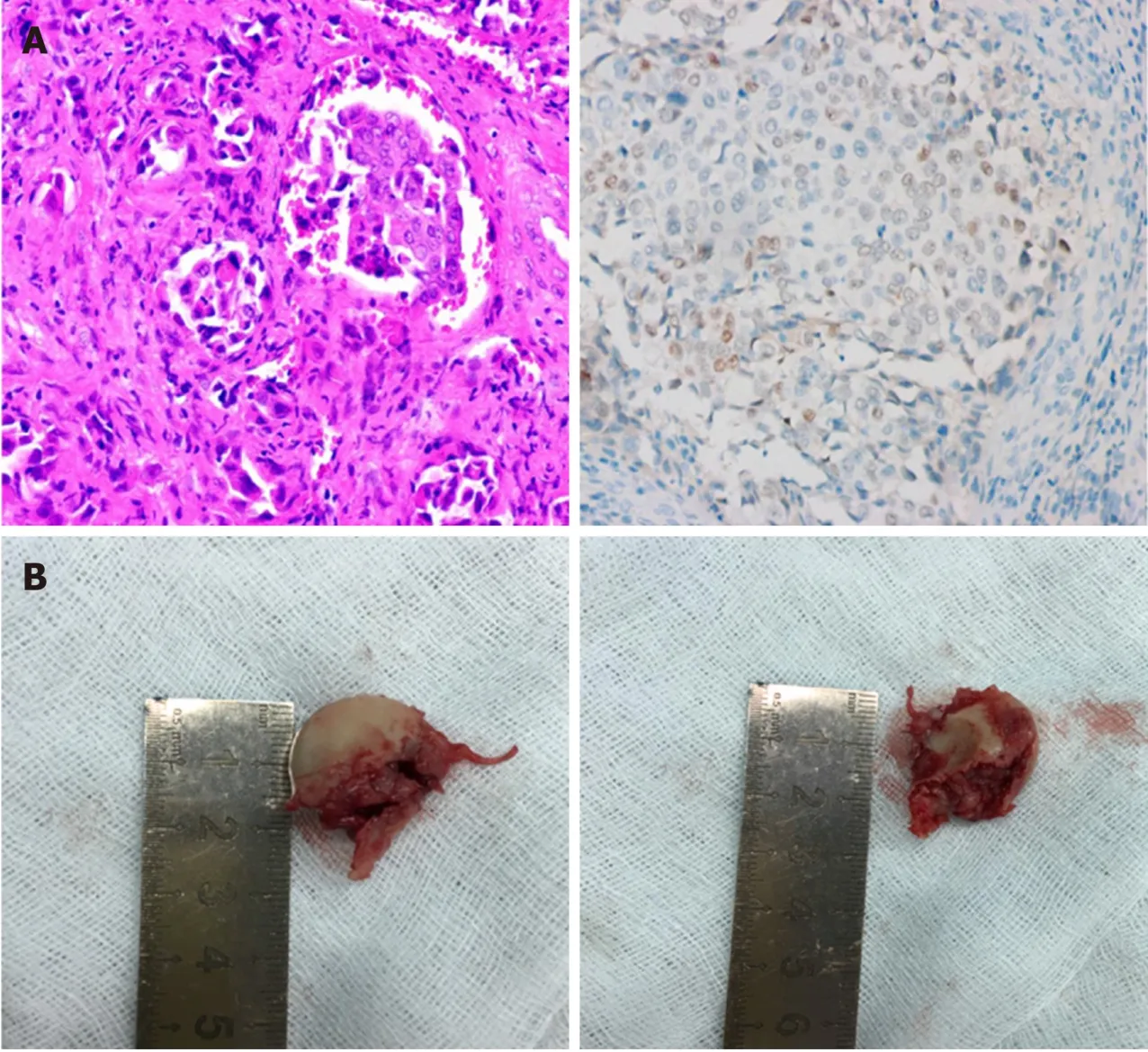
Figure5 lntraoperative photographs and postoperative pathological results.
 World Journal of Clinical Cases2020年7期
World Journal of Clinical Cases2020年7期
- World Journal of Clinical Cases的其它文章
- CD56+ lymphoepithelioma-like carcinoma of the lung:A case report and literature review
- Systemic treatment for severe concentrated sulfuric acid burns in an adult male at high altitude:A case report
- Clinical effects of apatinib mesylate for treatment of multiple brain micrometastases:Two case reports
- Disseminated histoplasmosis in primary Sj?gren syndrome:A case report
- Severe venous thromboembolism in the puerperal period caused by thrombosis:A case report
- Multiple neurofibromas plus fibrosarcoma with familial NF1 pathogenicity:A case report