Depression and myocardial injury in ST-segment elevation myocardial infarction:A cardiac magnetic resonance imaging study
2020-04-23 06:04:00ZhaoQingSunTongTongYuYueMaQuanMeiMaYunDiJiaoDongXuHeJiaKeWuZongYuWenXiaoNanWangYangHouZhiJunSun
World Journal of Clinical Cases 2020年7期
Zhao-Qing Sun,Tong-Tong Yu,Yue Ma,Quan-Mei Ma,Yun-Di Jiao,Dong-Xu He,Jia-KeWu,Zong-Yu Wen,Xiao-Nan Wang,Yang Hou,Zhi-Jun Sun
Zhao-Qing Sun,Tong-Tong Yu,Yun-Di Jiao,Dong-XuHe,Jia-KeWu,Zong-Yu Wen,Zhi-Jun Sun,Department of Cardiology,Shengjing Hospital of China Medical University,Shenyang 110004,Liaoning Province,China
Yue Ma,Quan-Mei Ma,Xiao-Nan Wang,Yang Hou,Department of Radiology,Shenyang 110004,Liaoning Province,China
Abstract
Key words: Depression;Patient Health Questionnaire-9;Myocardial injury;ST-segment elevation myocardial infarction;Cardiac magnetic resonance
INTRODUCTION
Patients with myocardial infarction (MI) have a high prevalence of depression[1,2].Post-MI depression has been independently associated with higher all-cause mortality,cardiac mortality,nonfatal events and health care costs[3-11].Altered autonomic nervous system activity[12],inflammation[13],platelet activation[14]and low brain-derived neurotrophic factor[15]may play important roles in the mechanism of depression affecting the prognosis of patients with MI.However,the detailed pathophysiological association between depression and adverse outcomes in patients with MI still needs further evaluation[16].Cardiac magnetic resonance (CMR) is the gold standard for quantifying post-MI myocardial injury[17,18].CMR-related variables,such as infarct size[19],microvascular obstruction (MVO)[20,21],area at risk (AAR)[22],intramyocardial hemorrhage (IMH)[23,24]and the myocardial salvage index (MSI)[25,26]are strong predictors for left ventricular remodeling and outcome in patients with MI.To date,there are no CMR data in the literature on patients with ST-segment elevation myocardial infarction (STEMI) and depression.The Patient Health Questionnaire-9(PHQ-9) is a self-report checklist derived from the interview used in the Primary Care Evaluation of Mental Disorders[27].The PHQ-9 assesses the presence and severity of depressive symptoms[28]and has reasonable sensitivity and specificity for patients with MI[29-33].Other studies have also found that the PHQ-9 could identify cardiac patients at risk for adverse cardiovascular outcomes[34,35].In this study,we aimed to assess the association between depression identified by the PHQ-9 and myocardial injury measured on CMR in patients with STEMI.
MATERIALS AND METHODS
Study design and setting
A total of 206 patients with STEMI admitted to Shengjing Hospital of China Medical University,Shenyang,China for primary percutaneous coronary intervention (P-PCI)were prospectively enrolled between November 1,2016,and November 1,2018.The diagnosis of STEMI should meet the following criteria to be eligible for P-PCI:(1)Chest pain present less than 12 h from onset of pain to time of catheterization;and (2)Significant ST-segment elevation (at least 0.1 mV in two or more standard leads or at least 0.2 mV in two or more contiguous precordial leads) or a new left bundle branch block.P-PCI was urgently undertaken according to the current guidelines[36,37].Clinical data and procedural data of all cases were obtained by the investigators using electronic medical records,interventional imaging data (Picture Archiving and Communication Systems technology;Neusoft,Shenyang,China),and surgical records.The exclusion criteria were as follows:(1) No depression data (12 cases);(2)No or poor-quality CMR data (72 cases);(3) Known malignancy,severe organic failure such as end-stage liver or renal failure (4 cases);(4) Significant cognitive dysfunction,including dementia and/or stroke,or antipsychotic treatment including antidepressant drugs at the time of evaluation (2 cases);and (5) Contraindications for CMR (e.g.,pacemaker or aneurysm clips) or contraindications for gadolinium-based contrast (e.g.,creatinine clearance ≤ 60 mL/min/1.73m2) (7 cases).A total of 107 patients with STEMI undergoing CMR were ultimately included in this study (Figure 1).This study complied with the Declaration of Helsinki,and the Shengjing Hospital of China Medical University Research Ethics Committee approved the research protocol.Written informed consent was formally obtained from all participants.
Depression measures
Depressive symptoms were assessed using the PHQ-9 three days post-MI and before discharge.The PHQ-9 is a brief depression screening instrument that patients are able to complete quickly and without assistance.It includes 9 items:(1) Lack of interest;(2)Depressed mood;(3) Sleeping difficulties;(4) Tiredness;(5) Appetite problems;(6)Negative feelings about self;(7) Concentration problems;(8) Retardation;and (9)Suicidal ideation.Patients were asked to what extent the symptom was present during the last 2 wk (0 = not at all;1 = on several days;2 = most of the time;3 = all of the time).A score between 0 and 27 points was obtained by the sum of the patient's responses.A PHQ-9 score of ≥ 10 has been recommended to screen for the diagnosis of major depression[27,28].
CMR imaging
According to the previous studies[17,18],CMR was performed at a median of 3 days (3-7 d) after P-PCI using a 3.0-T MR scanner (Philips Intera,Best,the Netherlands) with a 32-channel phased-array receiver coil.Images were ECG triggered and obtained during breath-holding at end-inspiration.Cine MR imaging was performed with a steady-state free procession cine sequence in the vertical and horizontal long-axis and short-axis of cardiac orientations.After the cine imaging,T2-weighted imaging with fat suppression was performed in the continuous short-axis orientation using a darkblood inversion recovery fast-spin echo sequence.Late gadolinium enhancement imaging was then performed 10 min after intravenous injection of 0.2 mmol/kg gadodiamide hydrate,using an inversion-recovery technique.
Physicians who were blinded to all clinical data performed the CMR analysis using a dedicated cardiac software package.Image quality was graded on a 4-point scale:3= excellent,2 = good,1 = moderate,and 0 = unanalyzable.The structural and functional parameters of the left ventricle were analyzed from cine imagesimaging on a commercially available workstation (MASS v7.2,Medis,City,The Netherlands).
AAR was defined as hyperenhancement (myocardial edema) on T2-weighted imaging,and expressed in grams and as a percentage of the total LV mass.Areas of hypoenhancement with edema were regarded as IMH and included in the AAR.Infarct myocardium was defined as the enhanced area of myocardium on late gadolinium enhancement images.The infarct size was expressed in grams and as a percentage of the total LV mass.Areas of hypoenhancement within the infarct were regarded as MVO and included in the infarct size.The myocardial salvage index was calculated as follows:(AAR-infarct size)/AAR.
Statistical analysis
Quantitative variables with a normal distribution were represented as the mean ± SD and compared with the independent samplest-test.Quantitative variables without a normal distribution were represented as median [interquartile range,(IQR)] and compared with Mann-WhitneyU-test.Categorical variables were represented as counts and proportions (%) and compared with theχ2test.Correlations between depression identified by the PHQ-9 and myocardial injury measured on CMR were assessed using Pearson's or Spearman's methods.Depending on the quintile of the infarct size,a large infarct size was defined as a value in the fifth quintile (infarct size≥ 20.94%).A binary logistic univariate regression analysis was performed to evaluate predictors of the infarct size.A binary logistic multivariate regression model was used to identify independent predictors of the infarct size.Variables withP< 0.05 in Supplementary Table 1 on univariate analysis were entered into a multivariate analysis.The results were reported as odds ratios (ORs) with associated 95%CIs.All tests were two-sided,and statistical significance was defined asP< 0.05.All statistical analyses were performed with SPSS version 19 (SPSS Inc.,Chicago,Illinois,United States).

Figure1 Correlation analysis between Patient Health Questionnaire-9 and infarction size,area at risk and myocardial salvage index.
RESULTS
Baseline characteristics of the patients by PHQ-9 score
A total of 107 patients with STEMI and CMR undergoing PCI were included in this study.Among them,19 cases (17.8%) had a PHQ-9 score of ≥ 10 and were diagnosed with major depression.As shown in Table 1,the major depression group had significantly higher heart rates on admission,higher creatinine and higher total cholesterol compared with the group of patients with a PHQ-9 score < 10.The percentage of intra-aortic balloon pump use was significantly higher in the major depression group.The major depression group also had a significant tendency towards decreasing stroke volume but increasing area at risk and infarction size(Table 2).
Prognostic performance of PHQ-9 to predict large infarction size
The univariate analysis found that multiple variables had significant effects on large infarct size:Troponin-I,high-density lipoprotein,door-to-balloon time,culprit vessels,SV,LVEF,AAR,MVO,IMH and MSI (Supplementary Table 1).
In the univariate logistic regression analysis,when PHQ-9 was evaluated as a continuous variable,an increased PHQ-9 score was significantly predictive of a large infarct size (OR:1.191,95%CI:1.087-1.305,P≤ 0.001,for per 1 unit increase) (Table 3).After adjusting for covariates,the PHQ-9 was still associated with large infarct size:The large infarct size risk increased by 22.6% per 1 increase in PHQ-9 score (OR:1.226,95%CI:1.073-1.401,P= 0.003) (Table 3).
When categorized into two groups,PHQ-9 ≥ 10 (major depression) remained significantly predictive of large infarct size (Table 3).In the univariate logistic regression analysis,the major depression group had a substantially higher risk of large infarct size (OR:4.380,95%CI:1.520-12.619,P= 0.006) (Table 3).In the multivariable logistic regression analysis,the major depression group still conferred a significantly higher risk of large infarct size (OR:4.840,95%CI:1.122-20.868,P= 0.034)(Table 3).

Table1 Baseline characteristics of the patients by Patient Health Questionnaire-9 score
Correlation analysis between PHQ-9 and myocardial injury indexes
The PHQ-9 score had a significant positive correlation with IS (r= 0.390,P≤ 0.001)and AAR (r=0.278,P= 0.004) but not with MVO,IMH and MSI (Table 4 and Figure 1).
DISCUSSION
The present study tested the association between depression identified by the PHQ-9 and myocardial injury measured on CMR in patients with STEMI undergoing PCI.The main findings were as follows:(1) PHQ-9 was an independent predictor of large infarction size;and (2) Depression could predict large infarction size in patients with STEMI undergoing PCI.
Frasure-Smithet al[3]first studied the prognostic value of depression among survivors of myocardial infarction.They found that depression was an independent risk factor for mortality at 6 months in 222 patients hospitalized following an MI,and its impact was equivalent to that of left ventricular dysfunction[3].This observation was then verified and extended by other studies and meta-analyses,which reportedthat post-MI depression was independently associated with higher all-cause mortality,nonfatal events and health care costs[4-11].In addition,other studies focused on the mechanism by which depression affects the prognosis of patients with MI[12-15].However,the detailed pathophysiological association between depression and adverse outcomes in patients with MI still needs further evaluation[16].
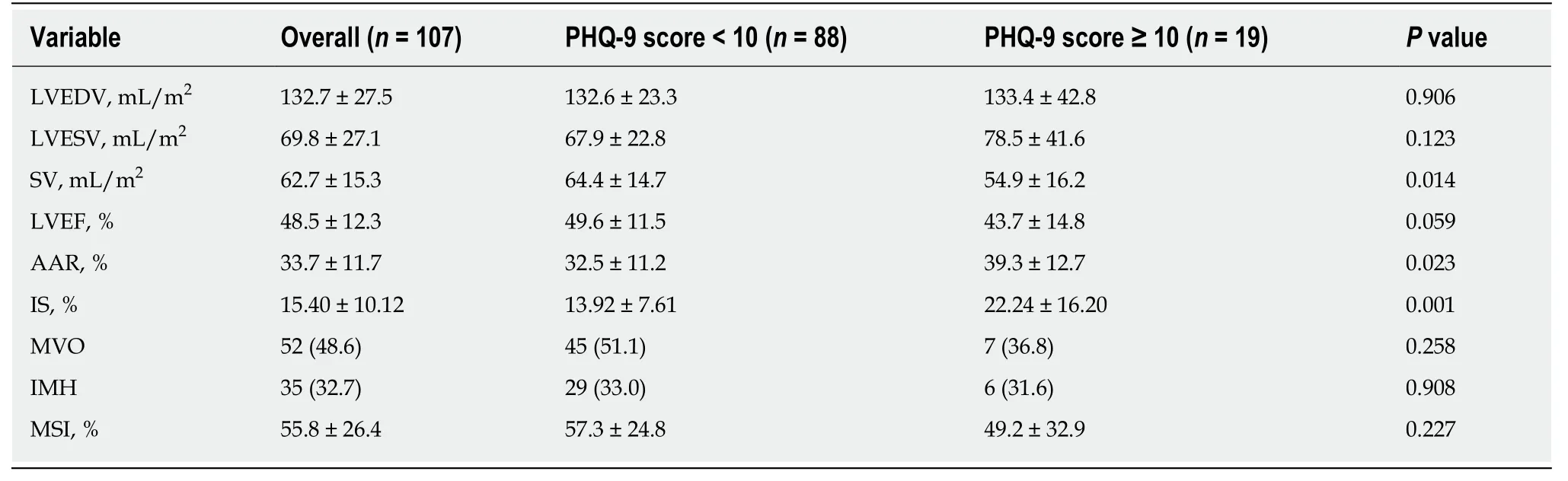
Table2 Cardiac magnetic resonance characteristics of the patients by Patient Health Questionnaire-9score
CMR can accurately quantify the structural and functional parameters of left ventricular and myocardial injury post-MI[17,18].Infarct size represents the total amount of myocardial infarction during STEMI.A previous study confirmed that infarct size,which was independent of left ventricular stunning and loading,was related to left ventricular remodeling and predicted future cardiac events[19].AAR,which is edematous myocardium at risk of infarction but still potentially reversible,is defined as an area of hyperenhancement (myocardial edema) on T2-weighted imaging.The extent of the AAR is predictive of an increased risk of cardiovascular events in patients with AMI[22].In this study,depression post-MI was associated with larger myocardial infarct and AAR evaluated by CMR.The results of this study provide a new pathological link to support the association of depression with adverse clinical outcomes.There is a possible explanation for this result.Acute coronary syndrome(ACS) patients with depression had higher levels of platelet micro particles and higher platelet aggregation to adenosine diphosphate and serotonin[14].Additionally,ACS patients with depression had higher plasma concentrations of platelet factor 4 and β thromboglobulin,which are secreted from alpha granules when the platelet is activated[38].Platelet aggregation plays a critical role in the formation of coronary thrombosis[39].Moreover,inflammation takes part in acute thrombotic complications such as plaque rupture and plaque erosion[40].Higher tumor necrosis factoralpha,IL-6,C-reactive protein levels and white blood cell count have been confirmed in ACS patients with depression[13,14],which indicates that depression may contribute to the maintenance of inflammatory responses.Taken together,depression may increase cardiovascular thrombosis through platelet activation and inflammation response.A greater extent of thrombus formation is related to a larger infarct size and AAR.This may provide a reasonable link between depression and adverse outcomes in patients with STEMI.
This study had several limitations.First,this study was prospective and observational,so potential confounders and selection bias could not be completely adjusted.Second,in this study,depression was assessed with a self-report questionnaire (PHQ-9) during patients' hospitalization and not with a formal psychiatric interview.However,previous studies have confirmed that the PHQ-9 could assess the presence and severity of depressive symptoms[28],and the PHQ-9 has reasonable sensitivity and specificity in patients with MI[29-33].Third,in this study,the time intervals between the onset of STEMI and CMR imaging were different,and the severity of myocardial injury may change over time post-MI[17,18].This was mainly because MRI examinations are in great demand but the machines are limited in our hospital,and it was difficult to ensure the same time interval.However,there was no significant difference in the time intervals between the two groups.
In conclusion,in patients with STEMI undergoing PCI,depression was independently associated with a large infarction size.The PHQ-9 may also help us assess myocardial injury in STEMI.

Table3 Effects of Patient Health Questionnaire-9 on large infarction size in the univariate and multivariate analyses

Table4 Correlation between Patient Health Questionnaire-9 score and myocardial injury variables measured on cardiac magnetic resonance
ARTICLE HIGHLIGHTS
Research background
Patients with myocardial infarction (MI) have a high prevalence of depression,which is related to poor prognosis.However,the detailed pathophysiology of this relationship is still unsubstantiated.Cardiac magnetic resonance (CMR) is the gold standard for quantifying post-MI myocardial injury.The Patient Health Questionnaire-9 (PHQ-9) could assess the presence and severity of depressive symptoms and has reasonable sensitivity and specificity for patients with MI.Revealing the pathological mechanisms underlying the association of depression with adverse clinical outcomes is still a main area of prognostic study of the cardiovascular field.
Research motivation
CMR is the gold standard for quantifying post-MI myocardial injury.Revealing the association between depression and myocardial injury measured on CMR may facilitate the detection of high-risk patients with MI and thereby improve the prognosis of patients.
Research objectives
This study aimed to assess the association between depression identified by the PHQ-9 and myocardial injury measured on CMR in patients with ST-segment elevation myocardial infarction (STEMI).
Research methods
A total of 107 STEMI patients undergoing primary percutaneous coronary intervention (P-PCI)were analyzed in this prospective cohort study.Each subject completed a PHQ-9 to assess the presence and severity of depressive symptoms.CMR was performed at a median of 3 d after PPCI for quantifying post-MI myocardial injury.Correlations between depression identified by PHQ-9 and myocardial injury measured on CMR were assessed.
Research results
The PHQ-9 was significantly predictive of large infarct size,and the major depression group had a substantially higher large infarct risk.The PHQ-9 score had a significant positive correlation with CMR-related variables of infarction size and area at risk.
Research conclusions
In patients with STEMI undergoing PCI,depression was independently associated with a large infarction size.The PHQ-9 may also help us assess myocardial injury in patients with STEMI.
Research perspectives
The results of this study provide evidence of a new pathological link to support the association of depression with adverse clinical outcomes of myocardial injury.In the future,more subjects should be incorporated to further confirm the results of this study.Mental health should be emphasized for cardiovascular disease patients.More importantly,cardiovascular physicians and psychologist should unite to fight against these diseases.
 World Journal of Clinical Cases2020年7期
World Journal of Clinical Cases2020年7期
- World Journal of Clinical Cases的其它文章
- CD56+ lymphoepithelioma-like carcinoma of the lung:A case report and literature review
- Systemic treatment for severe concentrated sulfuric acid burns in an adult male at high altitude:A case report
- Clinical effects of apatinib mesylate for treatment of multiple brain micrometastases:Two case reports
- Disseminated histoplasmosis in primary Sj?gren syndrome:A case report
- Severe venous thromboembolism in the puerperal period caused by thrombosis:A case report
- Multiple neurofibromas plus fibrosarcoma with familial NF1 pathogenicity:A case report