Acupuncture for premature ovarian insufficiency:a systematic review and meta-analysis
2020-02-28 08:46:06YinYaqian尹雅倩XuHuanfang許煥芳FangYigong房繄恭YangHuisheng楊會生LiXiaotong李曉彤ShangJie尚潔ZhengChensi鄭晨思HaoMingzhao郝鳴昭
Yin Ya-qian (尹雅倩), Xu Huan-fang (許煥芳),2, Fang Yi-gong (房繄恭),2, Yang Hui-sheng (楊會生), Li Xiao-tong (李曉彤),Shang Jie (尚潔), Zheng Chen-si (鄭晨思), Hao Ming-zhao (郝鳴昭)
1 Institute of Acupuncture and Moxibustion, China Academy of Chinese Medical Sciences, Beijing 100700, China
2 Acupuncture and Moxibustion Hospital of China Academy of Chinese Medical Sciences, Beijing 100700, China
3 Institute of Basic Research in Clinical Medicine, China Academy of Chinese Medical Sciences, Beijing 100700, China
4 China Press of Traditional Chinese Medicine, Beijing 100176, China
Abstract
Keywords: Acupuncture Therapy; Premature Ovarian Insufficiency; Meta-analysis; Systematic Review; Randomized Controlled Trials; Women
Premature ovarian insufficiency (POI) is a clinical syndrome defined by loss of ovarian activity before the age of 40 years old[1].It is characterized by menstrual disturbance (amenorrhea or oligomenorrhea) with raised gonadotrophins and low estradiol (E2)[2].Women with POI may present with typical symptoms of estrogen deficiency, including hot flash, night sweats,vaginal dryness, etc.The prevalence of POI is approximately 1% in the general population[1].POI can affect fertility, bone health, cardiovascular system,psychosexual, psychological and neurological functions,etc.Therefore, it demonstrates a signif icant negative impact on patients’ psychological wellbeing and quality of life (QOL)[1].
Hormone replacement therapy (HRT) is indicated for the treatment of low estrogen symptoms and the prevention of long-term health consequences of POI[1].However, HRT can’t improve ovarian activity, and a high relapse rate of the low estrogen symptoms is observed after drug withdrawal[3].Acupuncture, a form of traditional Chinese medicine (TCM) with a history of more than 3 000 years[4], has been used in China to regulate the female reproductive system for a long time[5].More and more studies have shown the effect of acupuncture in improving serum hormone levels in women with POI, and they described clearly the interventions in experimental and control groups which formed the basis of this systematic review and metaanalysis.
Ovarian reserve refers to a woman’s reproductive potential as a function of the quantity and quality of her remaining oocytes.The assessment of ovarian reserve is an essential part of the management of POI.Dynamic ovarian reserve tests assess the response of the hypothalamic-pituitary-ovarian (HPO) axis to a stimulus[6].The commonly used biomarkers of ovarian reserve are serum levels of follicle-stimulating hormone(FSH), luteinizing hormone (LH), E2, and anti-Müllerian hormone (AMH).As the number of ovarian follicles declines with age, both AMH and early follicular phase inhibin B concentrations decline[7].Decreased inhibin B secretion can lower the level of central negative feedback, resulting in an increased secretion of pituitary FSH and a higher concentration of late luteal and early follicular FSH[8].The earlier increase in FSH level stimulates an earlier onset of new follicular growth and an increase of E2level, which ultimately reduces the length of the follicular phase and the overall cycle.LH supports theca cells in the ovaries that provide androgens and hormonal precursors for E2production.At the time of menstruation, FSH is involved in follicular growth and has a specific effect on granulosa cells.With the rise in estrogens, LH receptors also expressed on the mature follicle, which causes it to produce more E2.Eventually, when the follicle is mature, a spike in progesterone production by the follicle inhibits the production of estrogens, leading to a decrease in the estrogen-mediated negative feedback of gonadotropinreleasing hormone (GnRH) in the hypothalamus, which then stimulates the release of LH from the pituitary[9].
Acupuncture has been used as a treatment for infertility for a long time, and there weren’t a lot of meta-analyses in this field.Thus, this systematic review aimed to assess the effect of acupuncture versus HRT for women with POI.
1 Methods
1.1 Criteria for recruiting studies
1.1.1 Types of studies
We included randomized controlled trials (RCTs) in Chinese or English published before January 31st, 2019.The types of trials included journal papers, conference papers and dissertations.Animal studies, qualitative studies, letters, news, editorials, and commentaries were excluded.
1.1.2 Participants
The diagnostic criteria of POI applied in this review included but were not limited to the testing and interpreting measures of ovarian reserve: a committee opinion (American Society for Reproductive Medicine 2015 Annual Meeting)[6]; European Society of Human Reproduction and Embryology (ESHRE) consensus on the definition of ‘poor response’ to ovarian stimulation forin vitrofertilization: the Bologna criteria[10]; the genetic basis of premature ovarian failure (Australian and New Zealand Journal of Obstetrics and Gynecology)[11];EuropeanSocietyforHuman Reproduction and Embryology(ESHRE)Guideline:Management of Women with Premature Ovarian Insufficiency(2015)[1]or the diagnosis in theGynecology of Traditional Chinese Medicine[12].
Women with POI who were under 40 years old and met the diagnostic criteria were included in this review.Those who had a history of ovarian surgery,radiotherapy/chemotherapy, congenital genital abnormalities, hysterectomy, bilateral ovariectomy or bilateral salpingectomy were excluded.
1.1.3 Types of interventions
We only included RCTs using acupuncture with needle insertion at acupoints, e.g., manual acupuncture or electroacupuncture (EA).Warm needling moxibustion is usually considered as a special method of acupuncture, so RCTs using warm needling moxibustion were also included.We excluded RCTs using ear-acupuncture, transcutaneous electrical acupoint stimulation (TEAS), acupoint application,catgut embedding, or bloodletting therapy.Trials involving acupuncture as an adjuvant to another treatment except HRT were also excluded.There were no limitations on acupuncture regimen (including acupoints, needling depth, time of needle retention,and treatment frequency), and characteristics of acupuncturist or acupuncture needle (brand or specification).
We included RCTs that compared acupuncture alone or acupuncture plus HRT with HRT alone.There were no limitations on characteristics of the involved HRT drugs,including ingredients, administration routes, dosage,dosage form, regimen, etc.
1.1.4 Types of outcome measures
The primary outcome was the basal serum level of FSH.The secondary outcomes were serum levels of LH,E2and AMH.
1.2 Search methods
1.2.1 Electronic search
This review was registered at the International Prospective Register of Systematic Reviews(CRD42018083903).The first search started in March 2018 after registration and was updated in January 2019.We searched for relevant studies in electronic databases comprising four Chinese databases: China National Knowledge Infrastructure (CNKI), Wanfang Academic Journal Full-text Database (Wanfang),Chongqing VIP Database (CQVIP), and Chinese Biomedical Literature Database (CBM), and four English databases: Web of Science, Cochrane Library, PubMed,and Excerpta Medica Database (EMBASE).Various combinations of MeSH headings and keywords were used, including two subsets.One subset was POI(‘premature ovarian insufficiency’, ‘primary ovarian insufficiency’, ‘menopause, premature’, ‘premature ovarian failure’, ‘amenorrhea’, ‘POI’, ‘POF’), and the other was acupuncture (‘acupuncture’, ‘acupuncture therapy’, ‘acupuncture points’, ‘meridians’, ‘needles’,‘electroacupuncture’, and ‘needling’).We restricted the search to studies in human.Taking PubMed as an example, the search strategies are listed in Table 1.
1.2.2 Data extraction and management
All studies were reviewed and selected independently by two reviewers (Yin Ya-qian and Shang Jie).The titles and abstracts were reviewed, and the articles which did not fit the eligibility criteria were excluded.If the title or abstract appeared to meet the eligibility criteria or we could not determine its eligibility,the full texts of the articles were obtained for further evaluation.Disagreements between the two reviewers were resolved by discussion and consensus with a third person.
We collected the following information from each included trial: study characteristics (e.g., authors, year of publication, article title, article type, the research methodology); participant characteristics (e.g.,diagnostic criteria, patient age, course of disease,sample size in each group); intervention characteristics(e.g., type, frequency of acupuncture, duration, HRT drug); and outcome measures.
1.2.3 Assessment of risk of bias in the included studies
Two authors (Yin Ya-qian and Li Xiao-tong)independently evaluated the risk of bias of the included studies.The risk of bias was assessed using the risk of bias assessment tool of the Cochrane Collaboration,which consists of 7 items[13]covering selection bias(random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective outcome reporting), and other sources of bias.Any discrepancies between the two reviewers were resolved by discussion with a third person (Yang Hui-sheng) until consensus was reached.
1.2.4 Data synthesis and analysis
Data were analyzed using RevMan version 5.3[13].We expressed the estimate of the effect as mean differences (MD) with 95% confidence interval (CI) for continuous outcomes, or as standardized mean difference (SMD) if the same outcome was measured at different scales.Pooled effects were estimated by meta-analysis if clinical heterogeneity was low.Statistical heterogeneity was evaluated using theI2statistics.The effect size was estimated with a fixed-effect model ifI2was below 50%.Otherwise, the random-effect model was used.Subgroup analysis was conducted based on the intervention type.All statistical analyses were performed using RevMan 5.3 software.A two-sided 5% level indicated statistical significance.If meta-analysis was inappropriate, a narrative summary of the results from individual studies was provided.
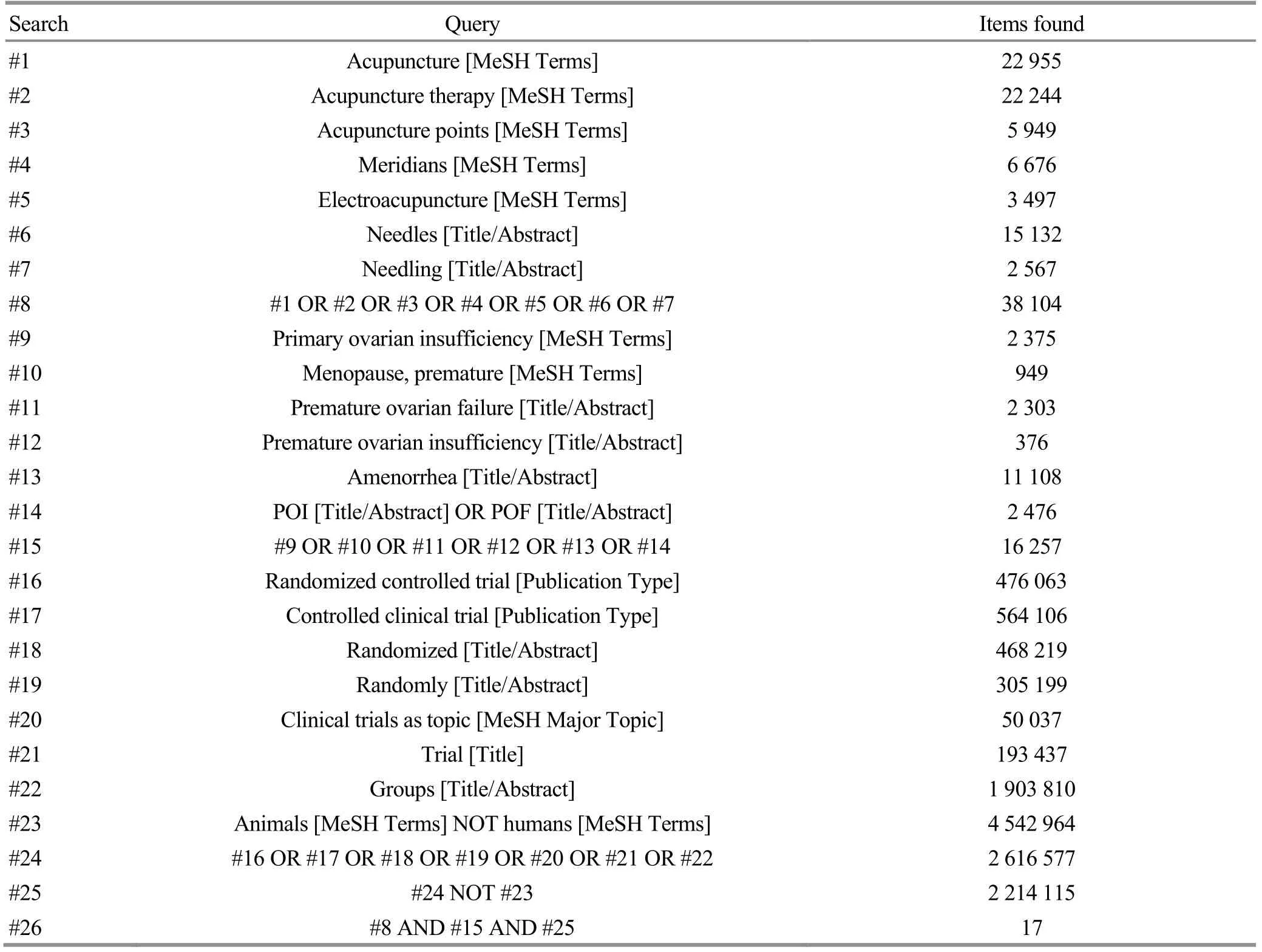
Table 1.Search strategies for PubMed
2 Results
2.1 Description of studies
Our initial search yielded 657 citations.We removed 276 duplicate records and rejected 337 irrelevant studies by checking the titles and abstracts according to the inclusion and exclusion criteria.Forty-four studies were retrieved and reviewed in full text, of which 36 articles were excluded.Finally, eight studies[14-21]including 496 POI patients were included in this review(Figure 1).
The characteristics of the included studies are shown in Table 2.One research[21]used three types of interventions: EA alone, EA combined with Chinese medicine and HRT alone.For this research, we only analyzed the data of EA alone and HRT alone.
2.1.1 Description of participants
The inclusion and exclusion criteria for participation were quite explicit for all the included studies.Judged from each reported diagnostic criteria, seven[14,16-21]of the eight included studies focused on the POI patients with FSH >40 IU/L, and one[15]focused on patients with FSH <40 IU/L.
2.1.2 Description of interventions
Six studies compared acupuncture and HRT[15,17-21].Two studies compared acupuncture plus HRT and HRT[14,16](Table 2).
2.1.3 Description of outcomes
As shown in Table 2, the basal serum level of FSH was used as an outcome measurement in all the 8 included studies.The secondary outcome was serum E2level in 7 studies, followed by serum LH level in 4 studies.Serum AMH level was used for effect assessment only in one study.
2.2 Risk of bias in the included studies
Risk of biases of the included studies was assessed using the Cochrane risk of bias tool[13].Three of the eight studies reported the use of random number table[14-15,21], while the rest studies did not report the randomization method.Attrition bias was low in all the included studies.Due to insufficient information, the risk of biases associated with allocation concealment,blinding and reporting and other possible biases were unclear (Table 3).
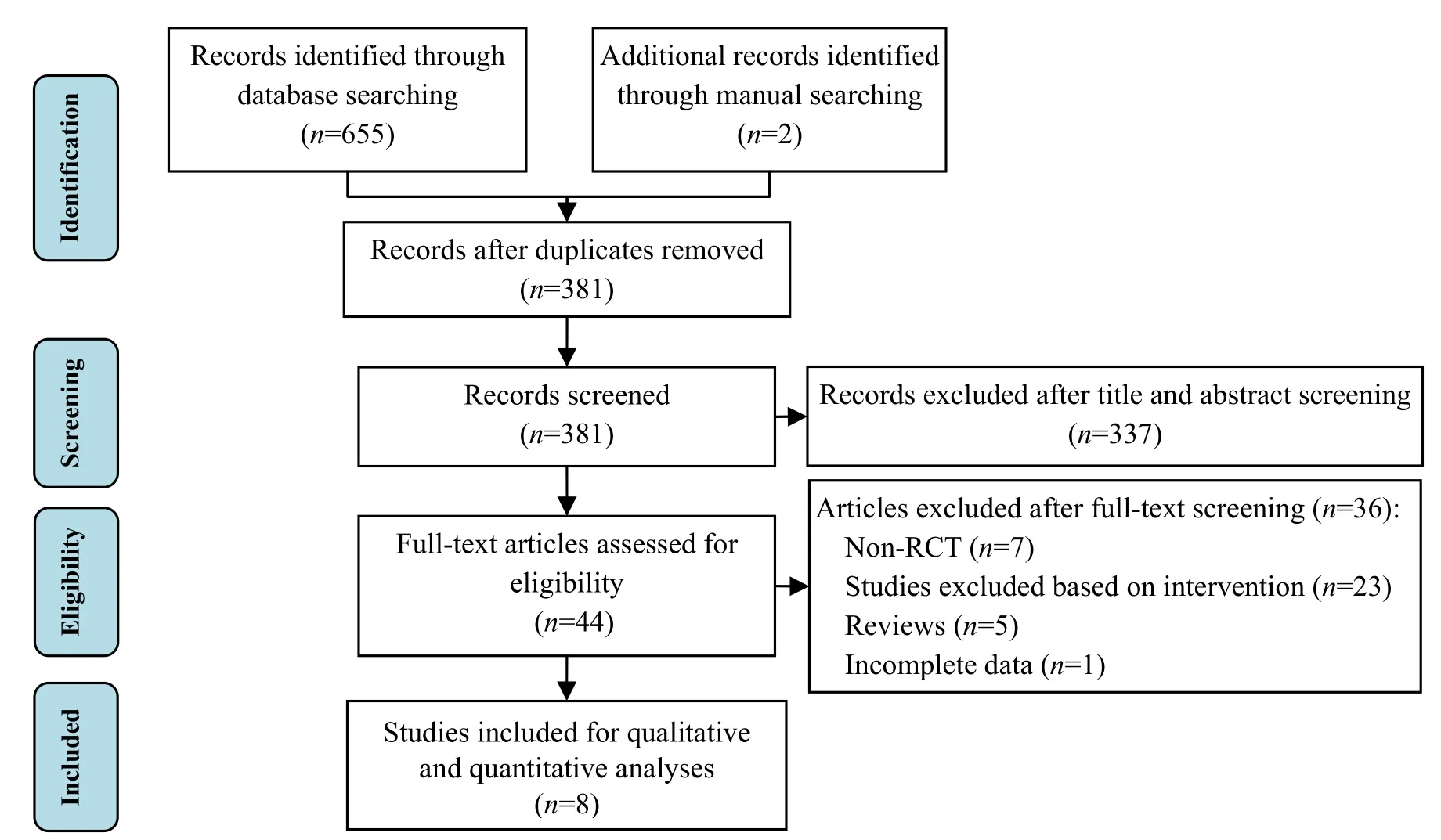
Figure 1.Flow chart of study selection
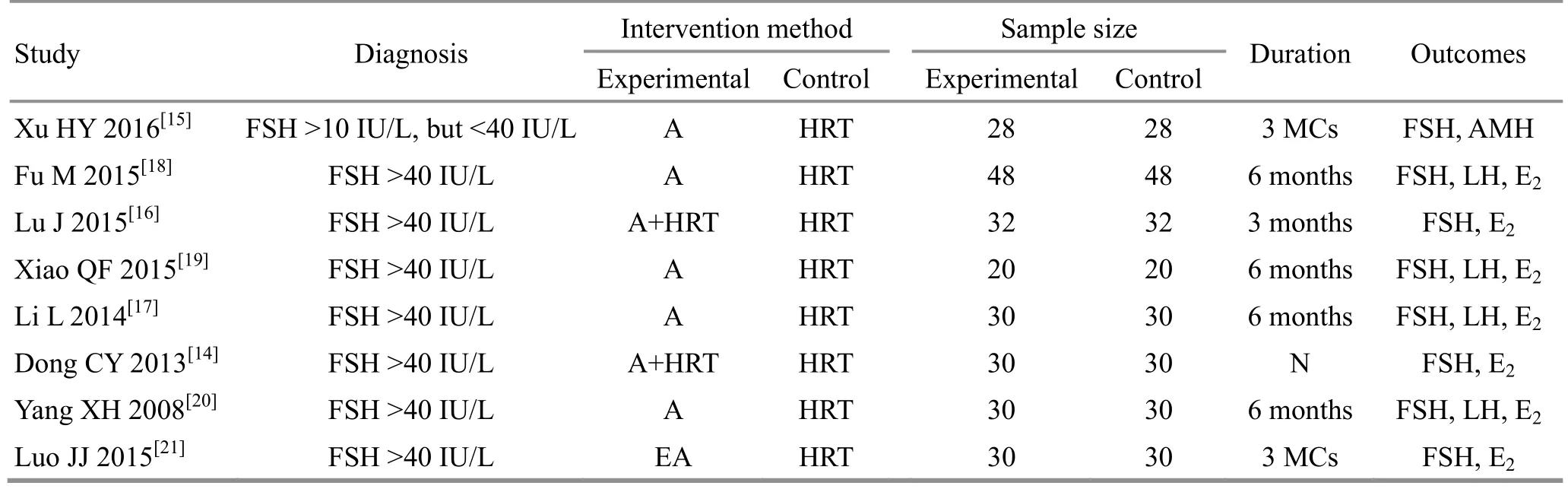
Table 2.Characteristics of the included studies
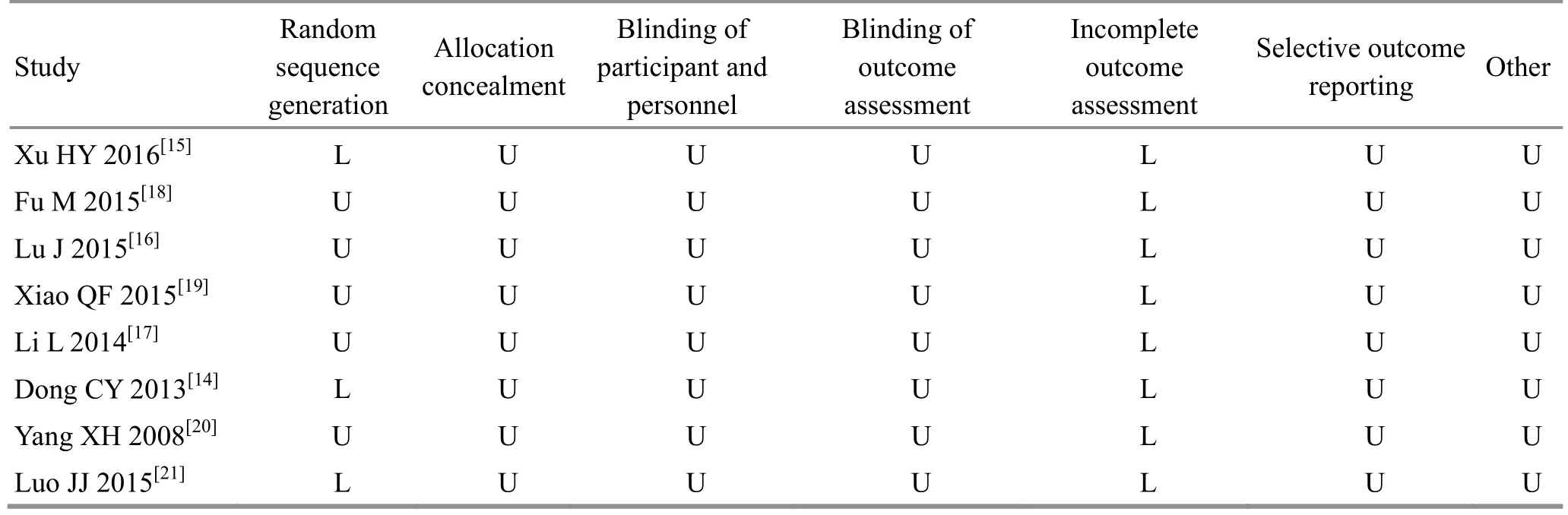
Table 3.Risk of bias summary
2.3 Primary outcome: serum FSH level
All the included studies assessed serum FSH levels after treatment.But there was considerable heterogeneity (I2=82%) across studies.The heterogeneity test on these 8 articles showedP≤0.1 andI2≥50%.Then we re-evaluated clinical methodology in the included studies and different interventions may be the source of heterogeneity.Further subgroup analysis was performed based on various interventions for the origin of heterogeneity.Six studies[15,17-21]compared acupuncture alone with HRT, and the other two studies[14,16]compared acupuncture plus HRT with HRT alone in decreasing the FSH level in POI patients.The pooled results showed that compared with HRT,significant decrease in the FSH level was observed both in acupuncture alone (MD=-4.53, 95%CI: -8.96 to -0.10,I2=73%,P=0.04)and acupuncture plus HRT (MD=-9.60,95%CI: -17.60 to -1.61,I2=50%,P=0.02), (Figure 2).There was an apparent heterogeneity in the subgroup of acupuncture versus HRT, so we used the random effect model for combining effect.Comparing the results of the two subgroups, it was found that the heterogeneity mainly came from the intervention methods.
The pooled result from all the included studies showed that the serum FSH level of POI patients in the acupuncture group was lower than that in the HRT control group (MD=-5.82, 95%CI: -9.76 to -1.87,P=0.004), indicating that acupuncture achieved a better total effective rate.
The skewed distribution of the funnel plot indicated potential publication bias (Figure 3).

Figure 2.Effect of acupuncture versus HRT on the serum level of FSH
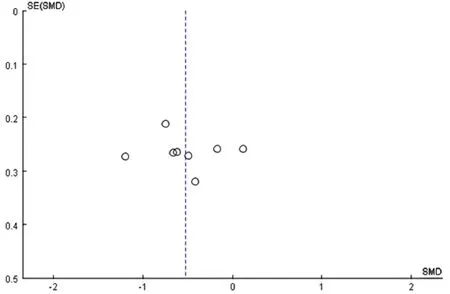
Figure 3.Funnel plot of reporting bias
2.4 Secondary outcomes
2.4.1 Serum LH level
Four studies[17-20]assessed the serum LH level using the same interventions (acupuncture versus HRT) after treatment.A high heterogeneity (I2=71%) was observed across studies (Figure 4).
Sensitivity analysis (Table 4) was used to address the heterogeneity.Clinical heterogeneity was observed in intervention types: one study[17]used conventional acupuncture, while the other three studies[18-20]used warm needling moxibustion.We also observed that one study[18]did not do acupuncture in the menstrual period, but the other three did acupuncture treatment continuously.After excluding the two studies mentioned above, we analyzed 2 studies using the fixed effect model, and combining effect was (MD=-3.16,95%CI: -9.41 to 3.10,P=0.32), (Figure 5).There was no significant change in combining effect after sensitivity analysis, suggesting a reliable outcome with low sensitivity.
2.4.2 Serum E2level
Seven studies[14,16-21]reported the serum level of E2.The pooled result showed that the serum E2level of POI patients in the acupuncture group was higher than that in the HRT control (SMD=0.93, 95%CI: 0.34 to 1.52,P=0.002).However, there was a high heterogeneity(I2=88%) across studies.Subgroup analysis showed that there was no significant difference between acupuncture alone and HRT (SMD=0.73, 95%CI: -0.01 to 1.47,I2=90%,P=0.05), while a remarkable elevation was found in acupuncture plus HRT when compared with HRT alone (SMD=1.43, 95%CI: 1.03 to 1.82,I2=0%,P<0.00001), (Figure 6).Sensitivity analysis also used to explore the source of heterogeneity, there wasn’t a significant change when we excluded study one by one in the subgroup of acupuncture alone and HRT, so the heterogeneity mainly came from the intervention methods.
2.4.3 Serum AMH level
Serum AMH level was reported in 1 study[15]comparing acupuncture alone with HRT.There was no significant difference in AMH between the two groups.
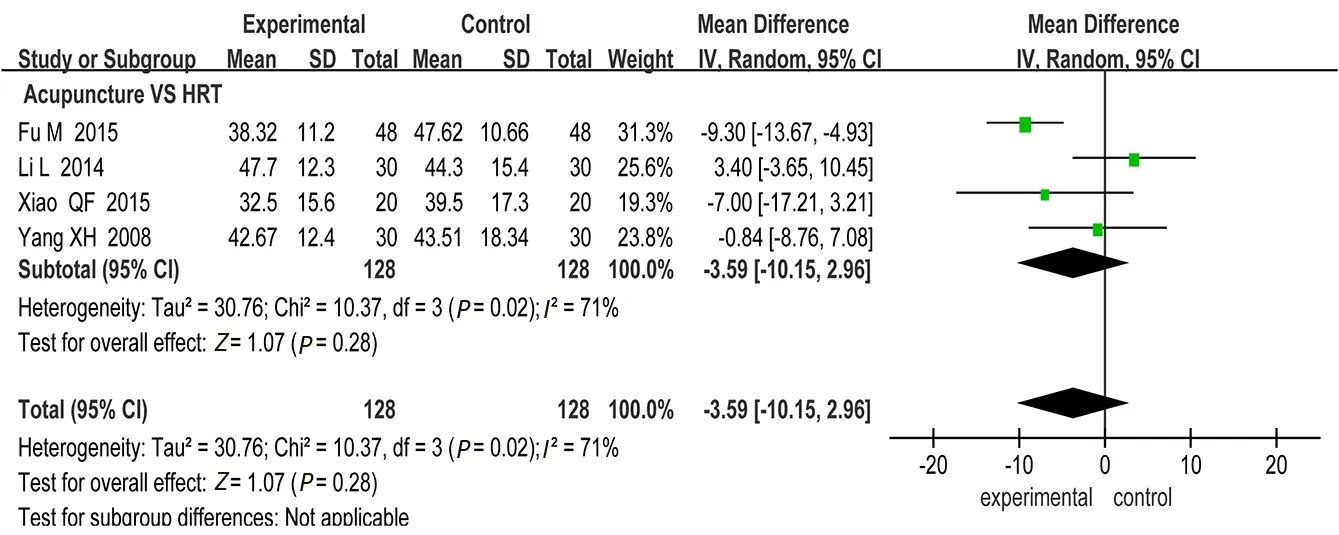
Figure 4.Effect of acupuncture versus HRT on the serum level of LH

Table 4.Studies for sensitivity analysis to explore the source of heterogeneity
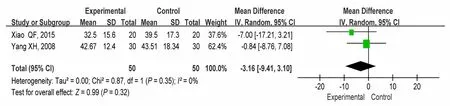
Figure 5.Effect of acupuncture versus HRT on the serum level of LH (2 studies)
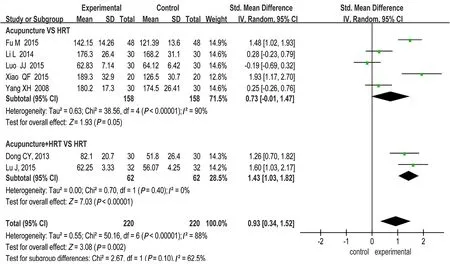
Figure 6.Effect of acupuncture versus HRT on the serum level of E2
3 Discussion
3.1 Summary of main findings
This systematic review and meta-analysis evaluated the effect of acupuncture versus HRT for women with POI.
In summary, limited evidences showed that acupuncture combined with HRT was better than HRT in reducing the serum FSH and increasing the serum E2level in POI patients, while acupuncture was not significantly different from HRT in improving the level of LH and AMH.
POI is characterized by cessation of ovarian function,and infertility and low estrogen are two key accompanying features for the diagnosis.Serum levels of FSH, LH and E2are commonly used to measure ovarian function.A high FSH level is associated with,though not necessarily predicting, both poor ovarian stimulation and the failure to conceive.Decreased FSH level can increase the opportunity for fertility.Low estrogen is closely related to vasomotor symptoms,vaginal dryness, and increased risk of bone loss or cardiovascular events, etc.The improvement of estrogen deficiency helps to improve the quality of life of POI patients.Our results showed the advantage of acupuncture over the control group (HRT) in lowering the serum FSH level and increasing the E2level, which was consistent with the results of a previous study[22],though in that study more interventions (including sham acupuncture, no treatment, or other active treatments) rather than HRT alone were adopted as controls.
Though AMH is considered as a more reliable and sensitive index for evaluating the ovarian function, few RCTs and no previous systematic review reported the results of AMH owing to its late application in clinical practice and research.
3.2 Limitations
There are several limitations in this review.First, the sample size was small, the quality was low and the overall risk of bias was unclear in each included study.Second, one study included some patients whose decline of ovarian function was less severe than POI,and that may bring bias to our study.Third, the recognized diagnostic criteria for POI were updated in December 2015 by ESHRE, in which the diagnostic threshold of FSH was reduced to 25-40 IU/L, however,none of the included studies used this criterion due to their early publication before or around 2015.Welldesigned RCTs recruiting POI patients diagnosed by 2015 ESHRE criteria are needed in future studies.
4 Conclusion
The present study indicated that acupuncture had an advantage over HRT in reducing the serum FSH and LH levels and increasing the serum E2level for women with POI.However, evidence supporting the finding is limited due to the small sample size, potential methodological flaws and significant heterogeneity.High-quality RCTs are required to confirm the effect of acupuncture for women with POI.
 Journal of Acupuncture and Tuina Science2020年1期
Journal of Acupuncture and Tuina Science2020年1期
- Journal of Acupuncture and Tuina Science的其它文章
- Initiation mechanisms of acupuncture effect: a literature review of basic studies
- Manipulation parameter optimization in Liu’s back tuina therapy for kids’ cough variant asthma in remission stage
- Clinical observation of sinew-regulating bone-setting manipulations plus exercise therapy for chronic non-specific low back pain
- Observation on therapeutic efficacy of tuina plus cupping for chronic fatigue syndrome
- Therapeutic efficacy and mechanism of heat-sensitive moxibustion for vascular dementia
- Clinical study on Jin’s three-needle therapy for post-stroke cognitive impairment