lmpact of pediatric inflammatory bowel disease diagnosis on exercise and sports participation: Patient and parent perspectives
2019-09-02 03:09:52RenMarchioniBeeryEnjuLiLaurieFishman
World Journal of Gastroenterology 2019年31期
Renée M Marchioni Beery, Enju Li, Laurie N Fishman
Abstract BACKGROUND Inflammatory bowel disease (IBD) may limit physical activity due to intestinal or extraintestinal manifestations, fatigue, or exercise perception. We sought to evaluate the influence of IBD diagnosis on exercise and sports participation in a pediatric population. We compared patient-reported and parent-reported perspectives.AIM To evaluate the influence of IBD diagnosis on exercise and sports participation in a pediatric population.METHODS Consecutive IBD outpatients (aged 10-18 years) and their parents completed parallel voluntary surveys. A validated, patient-reported functional activity scale,the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) was used to assess children's activity levels.RESULTS There were 149 completed surveys (75% response rate) with mean participant age of 16.5 years [standard deviation (SD) = 4.0] and mean age at IBD diagnosis of 11.8 years (SD = 3.4). Most patients (77%) were diagnosed within 12 mo of symptom onset. Current athletic participation was reported in 65% across 65 sports. Participation was greatest before (40%) rather than after (32%) IBD diagnosis, with no reported change in 28%. IBD negatively impacted play/performance in 45% but did not change play/performance in 44%. IBD treatment improved patients' desire to exercise (70%) and subjective capacity for aerobic exercise (72%). Patients and parents agreed that IBD subjects demonstrate normal capacity for aerobic exercise (0.40, 95%CI: 0.22-0.58) and that treatment improved both participatory desire (0.33, 95%CI: 0.12-0.54) and capacity for aerobic exercise (0.52, 95%CI: 0.31-0.71). Almost all (99%) viewed exercise as healthy, and most encouraged its practice. IBD patients demonstrated normal mean HSS Pedi-FABS scores.CONCLUSION After pediatric IBD diagnosis, most patients continue exercise and sports, with mean activity levels comparable to American youth. Treatment positively impacts participatory desire and aerobic capacity. Patients favor the role of exercise in IBD.
Key words: Inflammatory bowel disease; Physical activity; Exercise; Sports revised according to the STROBE Statement-checklist of items.
INTRODUCTION
Inflammatory bowel disease (IBD), encompassing Crohn's disease (CD) and ulcerative colitis (UC), is a chronic relapsing disorder of the gastrointestinal tract with multisystemic effects. As such, IBD may influence physical health and functionality due to disease-related factors such as abdominal pain, altered bowel habits, fatigue, and arthralgias or indirect factors such as time spent on medical visits, treatments, or hospitalizations. Psychological factors, including anxiety, depression and selfperception of wellness, can also contribute.
Exercise is recognized as a fundamental element for promoting general health and improved quality of life (QOL) among children and youth, including those with chronic diseases[1-3]. Physical activity and exercise participation in the context of IBD has been increasingly explored, although data is overall limited[4]. Exercise can contribute to improvement in IBD symptoms, disease activity and health-related QOL[5-10]. However, the disease may also restrict physical activity[11]. Youths' exercise habits prior to IBD diagnosis are often left out of the equation, and not all children were active before the diagnosis.
Our primary aim was to assess patient-reported exercise and sports participation both before and after IBD diagnosis to better understand the impact of disease on this important aspect of health. Survey questions explored past and current participation in various sports types, including non-organized physical play, organized sports, and competitive sports, across a range of academic years (elementary school through college). We sought to explore the particular factors affecting exercise and sports participation. Patients were asked about primary motivations and limitations for participation, and parents were asked to rank various barriers. Additional aims were to compare patient and parent perspectives on performance desire, perceived aerobic capacity, and the role of exercise in IBD. We obtained patient-reported activity levels using a functional activity scale.
MATERIALS AND METHODS
Study population
Surveys were distributed to consecutive pediatric IBD patients, aged 10-18 years,presenting for outpatient gastroenterology clinic or infusion center appointments at Boston Children's Hospital during a 3 mo time period. Each accompanying parent (or primary caregiver) was invited to participate in a parallel adult survey. All surveys were voluntary, anonymous and confidential, identified only by coded numbers and returned upon completion to the study team in a sealed envelope. The patient's submission of the survey implied consent. Parental consent was required for patients under age 18 years; parents could choose to complete or defer the adult survey.Exclusion criteria were inability to complete the survey in English or lack of parental consent.
Data collections
Surveys detailed exercise and sports participation before and after IBD diagnosis.Basic demographic data was collected on each subject including age, sex, IBD type,age at IBD diagnosis, and length of illness prior to formal IBD diagnosis. Survey questions examined participatory effort in casual or recreational physical play,organized sports, and competitive sports across each subject's range of academic years (elementary school, middle school, high school, and college). Questions explored how IBD diagnosis affected involvement in exercise and sports, considering both personal ability as well as the desire to play or perform. Subjects were asked if IBD treatment improved aerobic capacity or desire for physical activity. Parents had parallel questions about the influence of IBD diagnosis and treatment on their children's exercise practices. Parents were asked to rank the top three factors that limited patient participation. Free text questions asked subjects to describe the best and worst aspects of exercise and sports participation. A validated 8-item instrument,the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS), quantified activity levels and standardized them to those of United States children without chronic disease[12,13]. The HSS Pedi-FABS is a valid and reliable metric to evaluate activity level. It is not sport-specific but provides a generalizable measure of overall athletic activity over the previous month and records activity hours per week, endurance, level of competition, and degree of supervision of sports activity by trainers or coaches. The relationship between HSS Pedi-FABS score and patient age(categorized similarly to Fabricant et al[13]) was then examined.
Statistical analysis
Descriptive statistics were used to summarize patient demographics and clinical characteristics. Frequencies (%) were reported for categorical variables and means ±standard deviation (SD) were reported for continuous variables. To test if there was a difference across the three patient groups (reporting more, less, or same involvement in sports/exercise after IBD diagnosis), Analysis of Variance (ANOVA) was used for continuous variables; Chi-square testing was used for categorical variables. Sports participation and opinion variables were described in frequency (%), and Kappa coefficient was used to measure agreement of response between patients and parents.Patient-reported HSS Pedi-FABS scores were recorded to determine mean activity levels and compared across age groups. HSS Pedi-FABS data were scored from 0-30 and treated as a continuous variable for analysis. Multiple linear regression was used to assess whether there was an effect of age on HSS Pedi-FABS activity score after adjusting for sex and IBD type (CD vs UC). All analysis was performed using SAS 9.4;P values < 0.05 were considered statistically significant.
RESULTS
There were 149 completed surveys, representing a 75% response rate. Participants had a mean age of 16.5 years (SD = 4.0) with mean age at IBD diagnosis of 11.8 years (SD =3.4), and over half were male (57%). Patient-reported IBD subtypes included CD (77%)and UC (12%). Most patients (77%) reported symptoms for ≤ one year before IBD diagnosis. Patient characteristics are shown in Table 1.
Over 70% of children reported involvement in some form of exercise at various academic stages (elementary school, middle school, high school, and college), with more than half participating in organized or competitive sports (Table 2). The top 10 sports by academic stage are listed in Table 3. Almost two-thirds (65%) of patients reported participation over the previous year, across 65 sports. Factors that promoted participation included personal interest (71%), play of a friend (40%) or sibling (27%),and past participation of a father or mother (21% and 11%, respectively). The influence of a coach or teacher was small (5% and 2%, respectively), and only 7%reported participation due to school requirement.
Exercise participation was slightly higher before (40%) rather than after (32%) IBD diagnosis and did not change after diagnosis in 28%. Sex and type of IBD did not differ in these groups, but those who were more involved in sports after IBD diagnosis were diagnosed at a younger age compared to those reporting more involvement before diagnosis (10.6 years vs 12.6 years, P < 0.01).
IBD hindered play/performance in 45% but did not change play/performance in 44%. However, the majority of patients felt their activity level was at average or above; only 20% characterized their activity level as lower than average. The most frequently cited IBD-related reasons for diminished ability or desire for exercise/sports participation were tiredness/fatigue (22%) and abdominal pain (16%).IBD did not seem to affect type of sports participation, as only 18% reported there was a sport they would play if they did not have IBD. IBD treatment largely improved patients' desire to exercise (70%) and subjective capacity for aerobic exercise (72%).Total HSS Pedi-FABS activity score decreased with patient age but was not statistically significant in multivariate analysis; sex and IBD type were also not associated with activity score (Table 4).
Patients and parents agreed that IBD subjects: (1) Demonstrate normal capacity for aerobic exercise (0.40, 95%CI: 0.22-0.58); (2) Were more active before versus after IBD diagnosis [Kappa alpha = 0.67, 95% confidence interval (CI): 0.55-0.80]; and (3) Benefit from IBD treatment to improve both participatory desire (0.33, 95%CI: 0.12-0.54) and capacity for aerobic exercise (0.52, 95%CI: 0.31-0.71). Mean HSS Pedi-FABS activity score was 15 (of maximum 30 points).
Patient-reported best aspects of exercise/sports were: Health and wellness (31%),socialization/friendships/teambuilding (28%), fun/enjoyment (25%), and competition (16%); the worst aspects were: Physical symptoms such as tiredness/fatigue/illness-related symptoms (51%), competition (24%), time/commitment efforts (17%), and risk of injury (8%). Almost all patients (99%) viewed exercise as healthy (99%), and most (85%) advocated for its practice within the IBD population.
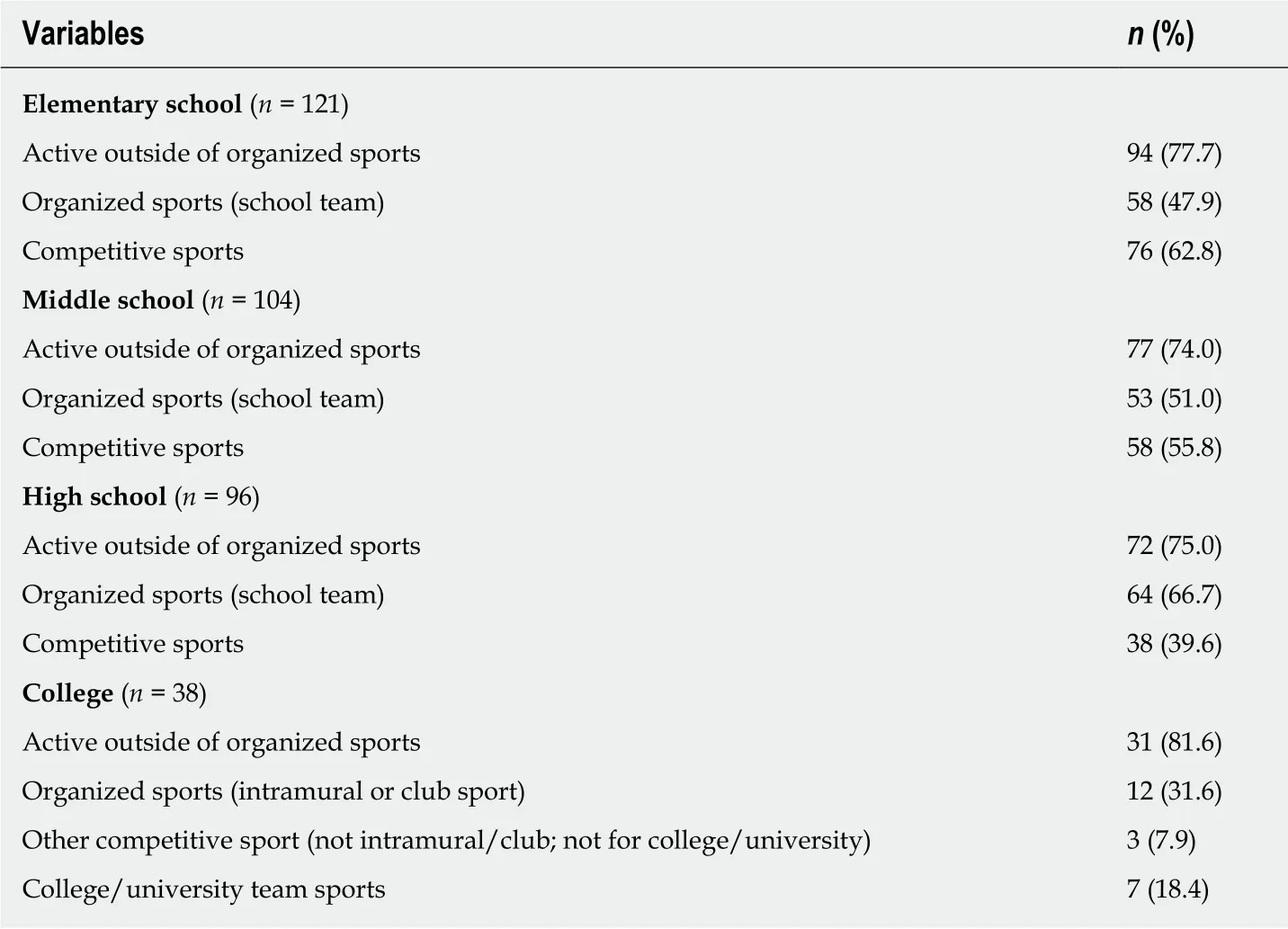
Table 2 Patient-reported exercise participation categorized by academic stage and activity type
DISCUSSION
This study is unique in assessing exercise and sports participation before and after IBD diagnosis in a pediatric IBD population. Many (65%) patients engaged in organized physical activity within the previous year, and this is in a group reporting 70% participation throughout the academic stages. The rate of competitive team play ranged from 40%-64%, and more than 65 sports were named. Only 18% reported that IBD prevented them from playing a sport they desired. Positive factors for participation included personal interest (71%) and participation by a friend (40%) or sibling (27%).
We found that patients and parents felt involvement in exercise and sports was greatest before rather than after IBD diagnosis, but the difference was small. The disease negatively impacted play/performance in 45%, while 44% were unaffected.Tiredness/fatigue and abdominal pain were identified as the main barriers to participation in our study, with no difference distinguished between IBD subtypes.Fatigue may be related to active inflammation, anemia, malnutrition, or depression;abdominal pain may reflect disease activity. A recent study in adults reported that IBD patients were significantly less physically active following IBD diagnosis,particularly for patients with UC[14]. Studies have identified weakness, fatigue, and abdominal pain as barriers to physical activity in adult IBD patients, even among those with low inflammatory markers and quiescent disease[15,16]. Bowel movement frequency and body image issues have also been identified but were not cited as barriers in our population[17,18]. A very limited number of subjects reported physical changes, such as surgical incisions, fistulas or scars, as limitations to play/performance. Further research can better characterize how these factors influence exercise in the pediatric IBD population. Understanding and addressing individual barriers to play/performance in the clinical setting can be useful to both caregivers and providers in order to appropriately advise for continued participation in physical activities.
Patients and parents in our population agreed on normal capacity for aerobic exercise in IBD, although it has been reported that pediatric patients with CD and UC may exhibit impaired aerobic and anaerobic exercise capacity regardless of disease duration or IBD activity[19]. Only 20% of patients felt their activity level was below average. Quantification of our IBD population's activity level yielded a mean HSS Pedi-FABS score of 15. This is similar to normative activity-level data (mean HSS Pedi-FABS score = 15.4) among American youth in the same age range, as established in a recent United States population-based study[13]. This study also found asignificant decrease in HSS Pedi-FABS activity scores with increasing age (r = -0.175, P< 0.001), corresponding to a linear decline in activity scores by an average of 27% from 10 years to 18 years[13].
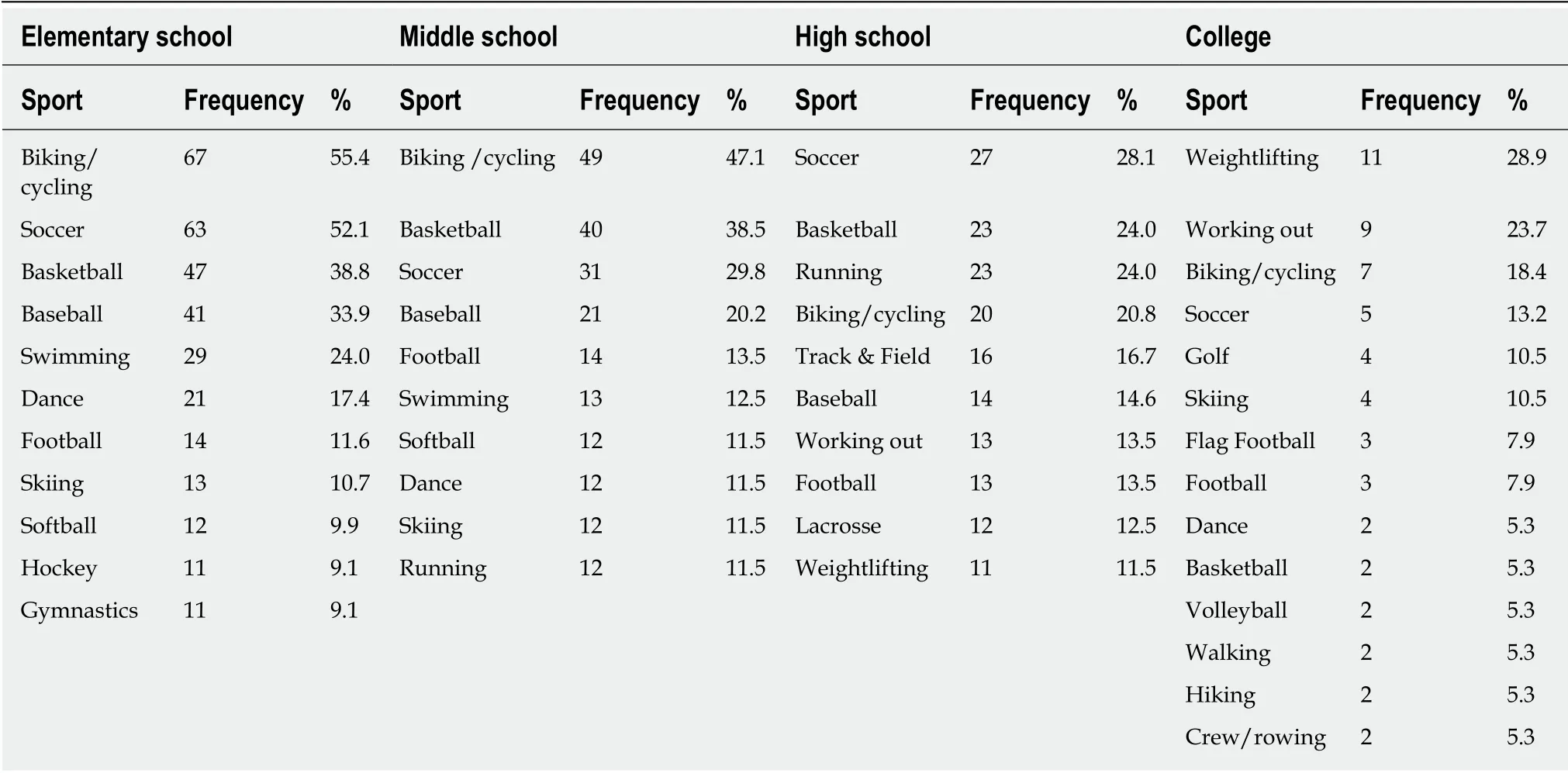
Table 3 Top 10 sports by academic stage
For patients with IBD who do not exercise, there can be a wide variety of explanations which should be further investigated. Severe IBD-related complexities including strictures or fistula, malnutrition/cachexia, prior surgery, presence of surgical wounds or an ostomy, infections, or hospitalizations may physically impede participation. Comorbid psychiatric disorders may limit the emotional drive to participate in exercise. Extraintestinal manifestations such as enteropathic arthritis or complications of metabolic bone disease such as osteoporosis or stress/fragility fractures may limit the ability to exercise safely or comfortably. Anemia secondary to chronic disease, iron deficiency, or enteric blood loss may contribute to fatigue and limited exercise capacity. Even with mild disease, anorexia and malabsorption may cause insufficient energy intake. A study of thirty-nine pediatric IBD patients with mild (n = 13) or quiescent disease activity (n = 26) revealed that lean body mass and physical activity were reduced compared to healthy age- and sex-matched controls[20].It is important to recognize that some children are just not interested in exercise and sports, regardless of the presence of IBD. For these children, encouraging and designing activity plans focused on individual choices and incorporating fun, varied,and non-intimidating physical activity with or without peers may foster motivation and social networks.
Our study has several limitations. This is a single-center study based at a quaternary medical center and thus may have limited generalizability. The severity of patient illness would typically be higher compared with lower acuity centers;therefore, the physical activity and sports participation in many other pediatric IBD care centers and community settings may be even higher. Patients who chose to participate in the survey may have had more interest in the topic of physical activity.Patient and parent surveys are subject to recall bias and, despite the anonymity,subject to social desirability bias. Self-completion of the HSS Pedi-FABS functional activity scale could overestimate athletic capability or underestimate it, particularly during a period of disease flare. We did not assess disease activity in correlation with exercise. Our comparison to the general healthy pediatric population is based on historical data rather than age-matched controls. Nonetheless, our study adds to the existing literature surrounding pediatric IBD, exercise, and sports participation.
In conclusion, the presentation of IBD in youth may be a particularly challenging scenario as a lifelong condition with unpredictable periods of flare and remission. Our study demonstrates that most patients with IBD remain active in exercise and sports,with only a small decrease in participation following diagnosis. Most of our pediatric IBD patients look favorably on the role of exercise and are currently involved and continue to partake in a variety of physical activities, with mean activity levels comparable to American youth. Treatment positively impacts participatory desire and aerobic capacity. Focusing treatment strategies toward the goal of “getting back in the game” may be a promising approach that encourages children and parents in the continued pursuit of various activities that can foster physical, mental and psychosocial aspects of health. Future studies are needed to establish physical activity targets in IBD patients based on individual disease factors and course.
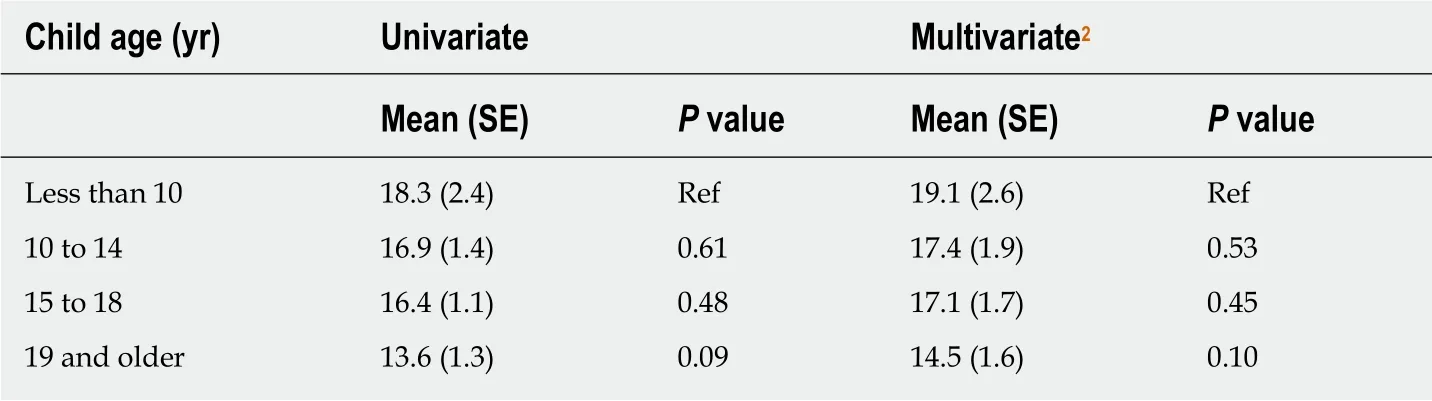
Table 4 Association between total activity score1 and patient age
ARTICLE HIGHLIGHTS
Research background
Inflammatory bowel disease (IBD), encompassing Crohn's disease and ulcerative colitis, may influence physical health and functionality due to a variety of disease-related factors such as abdominal pain, altered bowel habits, fatigue, and arthralgias or indirect factors such as time spent on medical visits, treatments, or hospitalizations. Psychological factors and self-perception of wellness may also contribute. Physical activity and exercise in the context of IBD has been increasingly explored, although data is overall limited.
Research motivation
Exercise is a fundamental element for promoting general health among children and youth,including those with chronic diseases. While exercise can contribute to improvement in IBD symptoms, disease activity, and health-related quality of life, the disease may also restrict physical activity. Additionally, youths' exercise habits prior to IBD diagnosis are infrequently considered. This survey was conducted to better understand the impact of pediatric IBD diagnosis on exercise and sports participation, considering both patient and parent perspectives.
Research objectives
The main objective of our study was to assess patient-reported exercise and sports participation both before and after IBD diagnosis. We sought to explore the particular factors affecting exercise and sports participation. Patients were asked about primary motivations and limitations for participation, and parents were asked to rank various barriers. Additional aims were to compare patient and parent perspectives on performance desire, perceived aerobic capacity, and the role of exercise in IBD. We obtained patient-reported activity levels using a functional activity scale.
Research methods
Consecutive IBD outpatients (aged 10-18 years) and their parents completed parallel voluntary surveys. Survey questions explored past and current participation in various sports types,including non-organized physical play, organized sports, and competitive sports, across a range of academic years (elementary school through college). A validated, patient-reported functional activity scale, the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) was used as a metric to assess children's activity levels.
Research results
There were 149 completed surveys (75% response rate) with mean participant age of 16.5 years[standard deviation (SD) = 4.0] and mean age at IBD diagnosis of 11.8 years (SD = 3.4). Most patients (77%) were diagnosed within 12 mo of symptom onset. Current athletic participation was reported in 65% across 65 sports. Participation was greatest before (40%) rather than after(32%) IBD diagnosis, with no reported change in 28%. IBD negatively impacted play/performance in 45% but did not change play/performance in 44%. IBD treatment improved patients' desire to exercise (70%) and subjective capacity for aerobic exercise (72%).Patients and parents agreed that IBD subjects demonstrate normal capacity for aerobic exercise(0.40, 95%CI: 0.22-0.58) and that treatment improved both participatory desire (0.33, 95%CI: 0.12-0.54) and capacity for aerobic exercise (0.52, 95%CI: 0.31-0.71). Almost all (99%) viewed exercise as healthy, and most encouraged its practice. IBD patients demonstrated normal mean HSS Pedi-FABS activity scores.
Research conclusions
This study demonstrates that most patients with IBD remain active in exercise and sports, with only a small decrease in participation following diagnosis. Most of our pediatric IBD patients look favorably on the role of exercise and are currently involved and continue to partake in a variety of physical activities, with mean activity levels comparable to American youth.Treatment positively impacts participatory desire and aerobic capacity.
Research perspectives
The presentation of IBD in youth may be a particularly challenging scenario as a lifelong condition with unpredictable periods of flare and remission. Focusing treatment strategies toward the goal of maintaining physical play or returning to exercise and sports may be a promising approach that encourages children and parents in the continued pursuit of various activities that can foster physical, mental and psychosocial aspects of health. Future studies are needed to establish physical activity targets in IBD patients based on individual disease factors and course.
 World Journal of Gastroenterology2019年31期
World Journal of Gastroenterology2019年31期
- World Journal of Gastroenterology的其它文章
- node dissection for low rectal cancer: ls it necessary?
- Layered enhancement at magnetic resonance enterography in inflammatory bowel disease: A meta-analysis
- Small bowel capsule endoscopy and treat-to-target in Crohn's disease: A systematic review
- Systematic review and meta-analysis of esophageal cancer in Africa:Epidemiology, risk factors, management and outcomes
- Application of indocyanine green-enhanced near-infrared fluorescence-guided imaging in laparoscopic lateral pelvic lymph node dissection for middle-low rectal cancer
- Ustekinumab: “Real-world” outcomes and potential predictors of nonresponse in treatment-refractory Crohn's disease