Multiline treatment of advanced squamous cell carcinoma of the lung:A case report and review of the literature
2019-08-14 07:43:00XinYangPingPengLiZhang
World Journal of Clinical Cases 2019年14期
Xin Yang,Ping Peng,Li Zhang
Abstract
Key words: Squamous cell carcinoma;Chemotherapy;Nab-paclitaxel;Anaplastic lymphoma kinase-targeted therapy;Antiangiogenic therapy
INTRODUCTION
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer death worldwide.According to the latest statistics,lung cancer represents 11.6% of the total new cancer cases and 18.4% of the total cancer deaths[1].Approximately 85%of all lung cancer patients have histological subtypes of non-small cell lung cancer(NSCLC),of which adenocarcinoma and squamous cell carcinoma (SCC) are the most common subtypes,having an incidence of 50% and 30%,respectively[2,3].Advanced NSCLC has a relatively poor prognosis,especially for those patients with stage IIIB/IV,with the overall 5-year survival being less than 5%[4].The SCC subtype is associated with even shorter survival than the nonsquamous NSCLC[5].
Herein,we report a case of advanced stage SCC involving a patient who was inoperable at the time of diagnosis.The patient underwent comprehensive treatment that included chemotherapy,radiotherapy,antiangiogenic therapy,and targeted therapy;today,at more than 5 years later,he remains alive.
CASE PRESENTATION
Chief complaints
The patient,a 45-year-old man,was referred to our hospital in April 2013 with complaints of a stuffy feeling in the chest,dyspnea,and pain in the right shoulder,without nausea,emesis,fever,or chills.
History of present illness
The patient reported the symptoms as having persisted for 1 mo,without exacerbating or relieving factors.
History of past illness
The patient reported no known systemic illness and no history of smoking or previous surgery.
Personal and family history
The patient reported no known relevant personal or family history.
Physical examination upon admission
Physical examination showed a body temperature of 36.8°C,breathing frequency of 19/min,pulse rate of 68 beats/min,blood pressure of 128/70 mmHg,performance status of 1,and lower breath sounds in the right lower lung.
Laboratory examinations
Laboratory examinations showed no obvious abnormalities.
Imaging examinations
Positron emission tomography/computed tomography imaging was performed on April 12,2013.Right lung cancer with right pulmonary,right pleural,mediastinal,and right hilar metastases was observed,along with right pleural effusion (Figure 1).Subsequent pleurocytology performed on April 19,2013 showed the presence of lymphocytes,mesothelial cells,and neutrophils.
Genetic testing
Thoracoscopic biopsy of right ventricular pleural metastases was performed on April 23,2013.The pathological result showed lowly-differentiated SCC of the chest wall(derived from the right lung) (Figure 2).Immunohistochemistry (Figure 2) analysis characterized the tumor tissue to be PCK (+),CK5/6 (+),p63 (+),and Ki-67 (+,≈ 30%)(Supplementary Figure 1).Genetic testing detected noEGFRmutation.
FINAL DIAGNOSIS
According to the collective findings,the patient was diagnosed with right lung SCC stage IV (metastases to the right lung,right pleura,and mediastinum and malignant pleural effusion),EGFRmutation-negative.
TREATMENT
DP chemotherapy,consisting of 75 mg/m2docetaxel on day 1 and 75 mg/m2cisplatin on day 1,was administered as first-line therapy,following the NCCN Guidelines V2.2013.After two chemotherapy cycles,the disease was evaluated on June 7,2013 and characterized as a progressive disease (Figure 3).TP chemotherapy,consisting of 100 mg/m2nab-paclitaxel (nab-PC) on days 1,8,and 15,and 75 mg/m2cisplatin on day 1,was used as second-line therapy starting on June 7,2013.After six cycles of this therapy,the tumor shrank significantly,as evidenced on November 22,2013 (Figure 3).
The patient’s condition remained stable over the next 2 years.At follow-up on June 9,2015,after 23.9 mo of progression-free survival (PFS),evaluation of the state again showed a progressive disease.We looked to the NCCN Guidelines and decided to treat with GP therapy,consisting of 1250 mg/m2gemcitabine on days 1 and 8,and 75 mg/m2nedaplatin on day 1,as the third-line therapy method.Unfortunately,the disease progressed after four cycles of GP and three cycles of gemcitabine monotherapy,as determined on January 11,2016,following a total 7.0-mo PFS.Although the fourth-line therapy of NVB + endo,consisting of 25 mg/m2vinorelbine on days 1 and 8,and 30 mg endostar on days 1-7,had a great effect on the disease,we had to discontinue the therapy after three cycles because of the intolerable gastrointestinal reactions.
For the next treatment method,we administered nab-PC again,considering the fact that the previous nab-PC had given the patient a total PFS of 23.9-mo.This time,nab-PC monotherapy also showed considerable efficacy after seven cycles of administration,giving a total PFS of 11.0-mo.Then,after careful and thorough evaluation,the patient started to receive radiotherapy in the right lung (DT = 50 Gy/5F) on April 27,2017.The tumor shrank,as predicted (Figure 4),but started to grow again after 6 mo.However,radiation-induced lung injury (RILI) was observced after the radiotherapy,accompanied by cough and shortness of breath.Corticosteroid-based therapy was administered to improve RILI.On January 23,2017,a percutaneous lung biopsy was taken and the pathological result indicated non-keratinized SCC.
Immunohistochemistry analysis showed positivity for anaplastic lymphoma kinase(ALK) D5F3,consistent with the result of blood gene testing,which indicated a rearrangement ofALK[i.e.,a gene fusion of SPTBN1-ALK (S27:A20)].Still,noEGFRmutation was found in the tissue gene testing.Thus,crizotinib was used in the next round of therapy,starting on February 2,2018.In July of that year,anlotinib was administered instead.
The entire process of treatment is presented along a timeline in Figure 5.
OUTCOME AND FOLLOW-UP
Up to now,the disease has remained stable in the patient.No obvious enlargement of the tumor was observed,and the RILI also improved,with some small focal fibrosis left.Long-term,regular follow-up is still in progress.The patient has also been advised to receive regular imaging examinations.
DISCUSSION
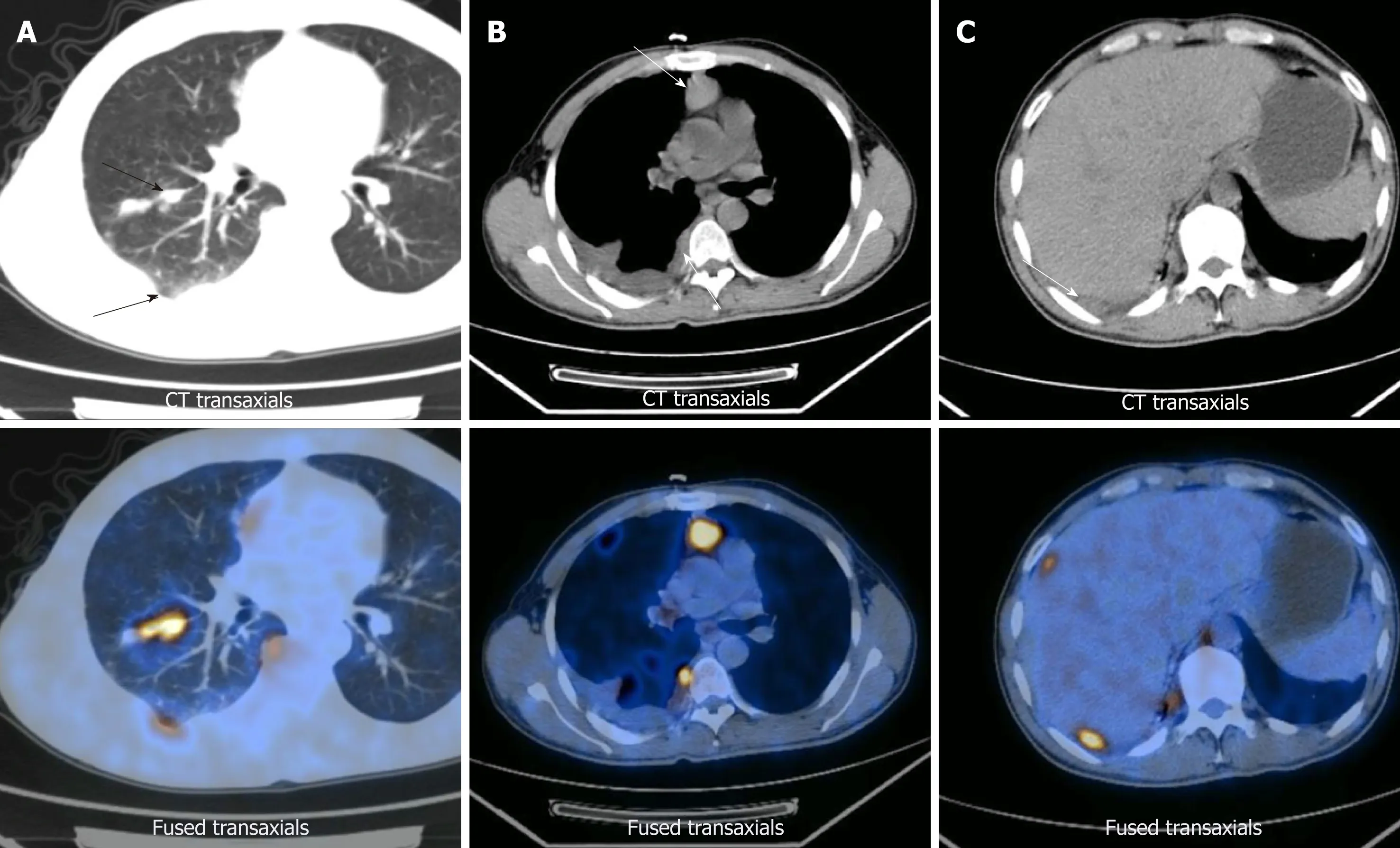
Figure1 Images from positron emission tomography/computed tomography preformed on April 12,2013.
Our patient was diagnosed with advanced SCC;multiple biopsies and gene testing offered us a whole and thorough understanding of the disease,so that we could administer an individualized comprehensive treatment that included chemotherapy,radiotherapy,antiangiogenic therapy,and targeted therapy.Multiline therapy made a great contribution to the patient’s survival,although the patient experienced multiline relapse.
Historically,the treatment for SCC has been mostly limited to cytotoxic chemotherapy because of the lack of targetable aberration.Currently,platinum-based chemotherapy is the mainstay of the first-line treatment in those patients without targetable aberration or with high-level expression of PD-L1,and platinum agents are most commonly administered with taxanes,gemcitabine,vinorelbine,or pemetrexed[6].Solvent-based paclitaxel plus carboplatin is the most frequently used taxane-platinum combination in the United States;reports cite a 15%-32% objective response rate and a median overall survival of 7.9-mo to 10.06-mo for this therapy[7].Nab-PC is a new type of paclitaxel,which is produced by binding paclitaxel to 130-nm albumin particles,aiming to overcome the solvent-associated limitations.Nab-PC has higher efficiency and fewer toxicities and can be provided to the patient more conveniently due to the fact that it does not require any solvents and eliminates the need for steroid pretreatment.
Some studies have shown that nab-PC elicits superior response rates compared with solvent-based paclitaxel in first-line therapy of patients with advanced NSCLC,especially for those with the SCC subtype[8,9].In those patients with SCC histology,a 68% improvement in objective response rate was achieved with nab-PC plus carboplatin,as compared to that with solvent-based paclitaxel plus carboplatin (41%vs24%,respectively).That result was inspiring since the basic treatment options for SCC at the time were limited[9].Several studies have also demonstrated the efficacy and tolerability of nab-PC as second-line or late-phase chemotherapy in advanced SCC[10-14].For our patient,nab-PC plus cisplatin was first administered as the secondline therapy,due to the patient’s poor response to the DP therapy;it showed considerable efficacy and led to a total PFS of 23.9-mo,without obvious adverse effects.Moreover,when subsequent therapy failed to provide a remarkable benefit,the nab-PC chemotherapy still showed efficacy.
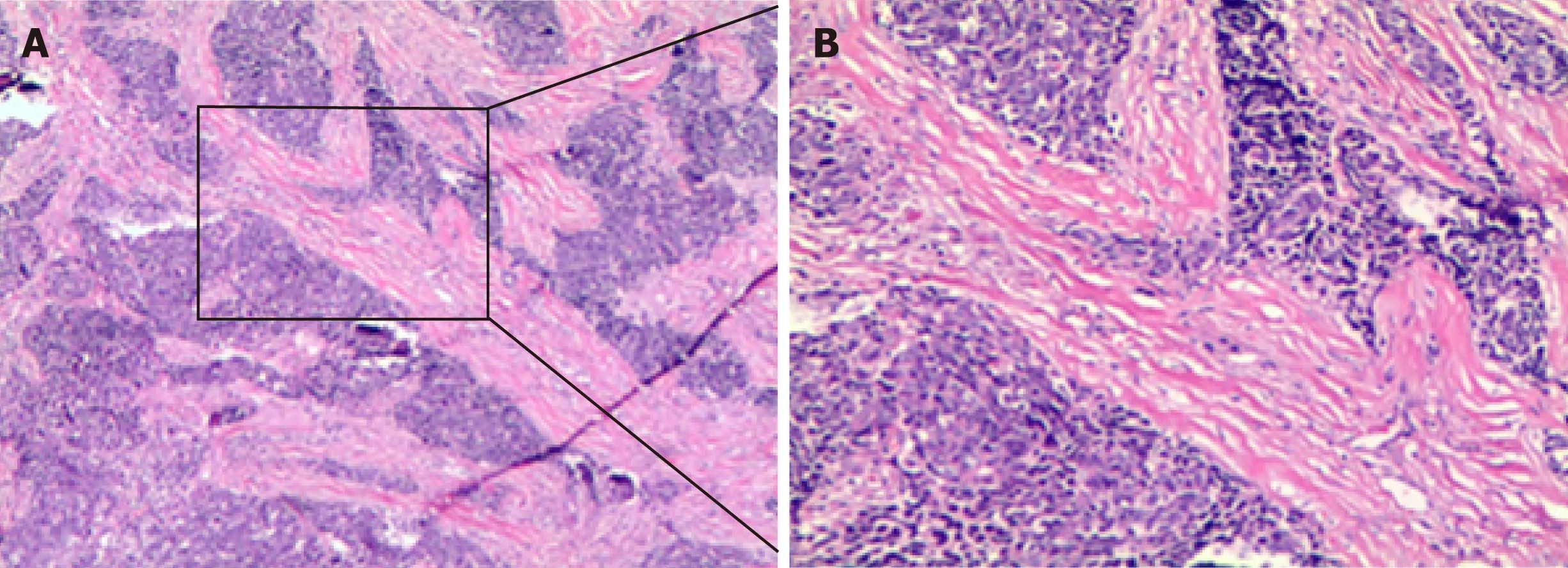
Figure2 Pathological findings on April 23,2013.
Radiotherapy is not only the main treatment method for early-stage NSCLC patients who are considered inoperable but also plays an important role in those patients with advanced lung cancer.Palliative radiotherapy is effective in improving thoracic symptoms,especially for those patients with advanced lung cancer[15,16];the positively impacted symptoms include hemoptysis,cough,chest pain,and dyspnea,thus improving the patients’ life quality.Besides controlling symptoms,palliative radiotherapy is also beneficial to patient survival.Several clinical trials have demonstrated the ability of radiotherapy to improve survival in patients administered with palliative intention for locally advanced lung cancer[17-19].Our patient received radiotherapy in the right lung after becoming resistant to chemotherapy;the tumor shrank,as predicted,offering the patient a PFS of 6-mo.
When radiotherapy was no longer useful,results of pathological analysis and blood gene testing indicated a gene fusion ofSPTBN1-ALK(S27:A20),leading to the administration of crizotinib therapy.Our patient then showed a response,although limited,to crizotinib therapy.Lung cancer with ALK-rearrangements are reliant upon ALK signaling and can be inhibited by ALK tyrosine kinase inhibitors (commonly referred to as TKIs).Crizotinib is an oral small-molecule TKI that targets ALK,MET,and ROS1 tyrosine kinases and has demonstrated considerable efficacy in several clinical trials[20,21].It was approved by the United States Federal Drug Administration in August 2011 for treatment of patients with advanced NSCLC andALKrearrangements.However,very little data has been reported on its use in patients with the SCC subtype andALKrearrangement[22].
The lack of these data in the literature may be due to the fact thatALKrearrangement is seen in only 1% of SCC cases ,and only about 5% of adenocarcinoma cases[22,23].Thus,it remains unknown whether or not those patients withALKrearrangement-positive SCC would benefit from TKIs like crizotinib.Several cases of SCC withALKrearrangement have been reported as well as cases with considerable responses to crizotinib therapy[24-26],even after failed chemotherapy[25];the associated PFS times reported are 6.0-mo,5.9-mo,and 7.0-mo,respectively.We attach importance toALKgene testing for patients with advanced SCC,as they may benefit from ALK-targeted therapy,let alone the more powerful drugs that are coming out.For example,compared with crizotinib,the new drug alectinib has shown superior efficacy and lower toxicity in the treatment of NSCLC withALKrearrangement[27,28].
Anlotinib is a new,orally administered multitargeted receptor TKI and has already shown a broad-spectrum antitumor potential.Several clinical trials have revealed the importance of anlotinib as a third-line or late-phase therapy in NSCLC[29-31].ALTER-0303 was a phase III trial that compared the efficacy and safety of anlotinib with those of placebo in patients with advanced NSCLC who had progressed after at least two lines of prior treatments[29];the result showed that,compared with placebo,anlotinib provided improvement in the objective response rate (9.18%vs0.7%,P< 0.0001) and prolonged the median survival rates,both for PFS (5.37 movs1.40 mo) and overall survival (9.63 movs6.30 mo).Subgroup analysis of the anlotinib-related histology revealed that when the drug was given as a subsequent therapy strategy,there was an improvement in PFS for both advanced adenocarcinoma and SCC cases[30].Anlotinib was approved by the China Food and Drug Administration for third-line treatment or beyond in advanced NSCLC on May 8,2018.We initiated anlotinib therapy with our patient in July 2018 and that treatment is ongoing to date.Importantly,efficacy has been observed through the latest follow-up appointment (in November 2018),without presentation of any obvious adverse effects.
CONCLUSION
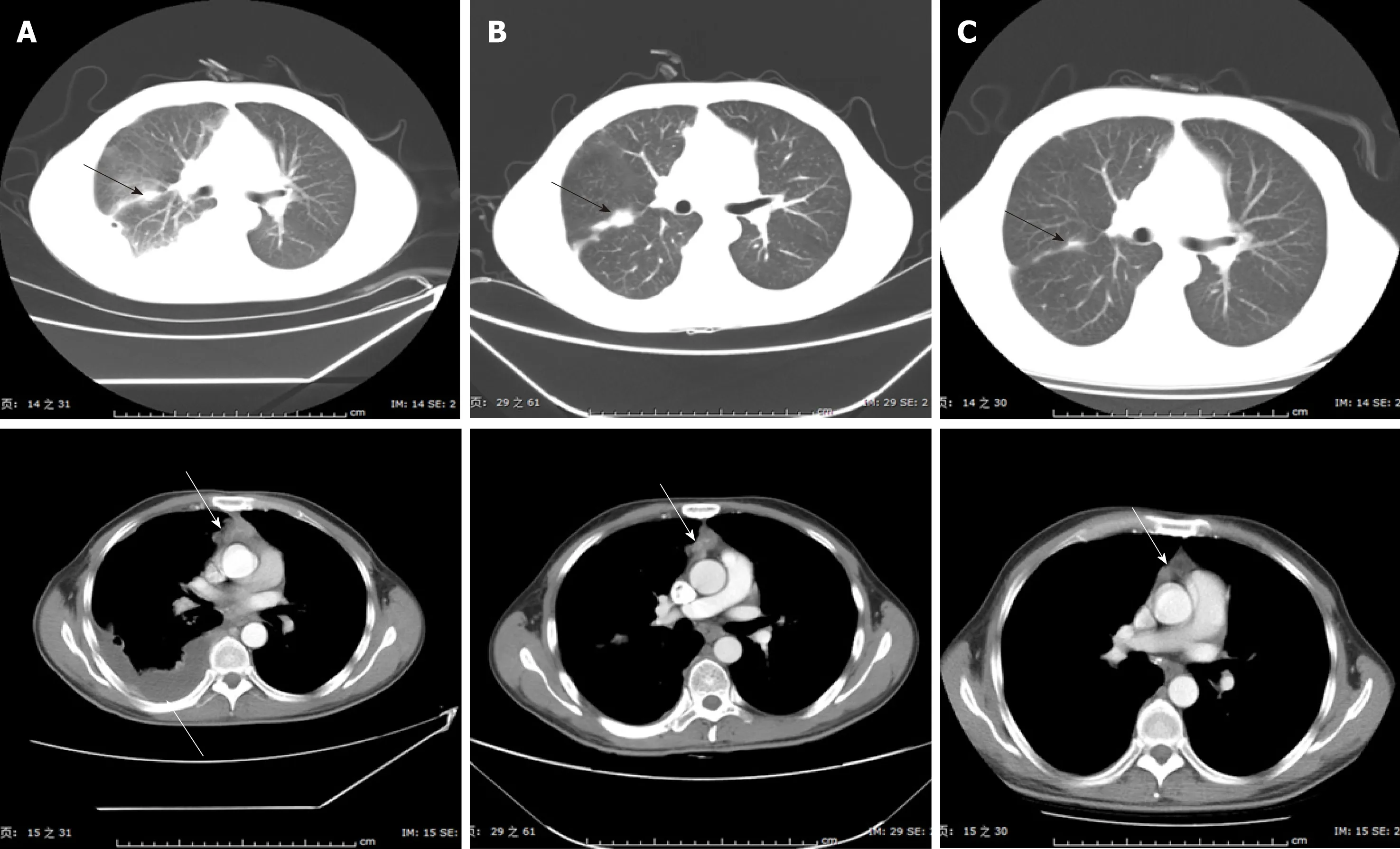
Figure3 Images from computed tomography showing the tumor in the right lung and mediastinum in response to therapy.
We present herein a case of advanced SCC treated by administration of multiline treatment.Throughout the entire process of the comprehensive treatment,the patient showed a remarkable response to the nab-PC-based chemotherapy,radiotherapy,ALK-targeted therapy,and antiangiogenic therapy,which also prolongs PFS and overall survival.We attach importance to individualized treatment and hope to focus the attention of clinicians towards the benefits of a flexible application of multiline therapy combination.
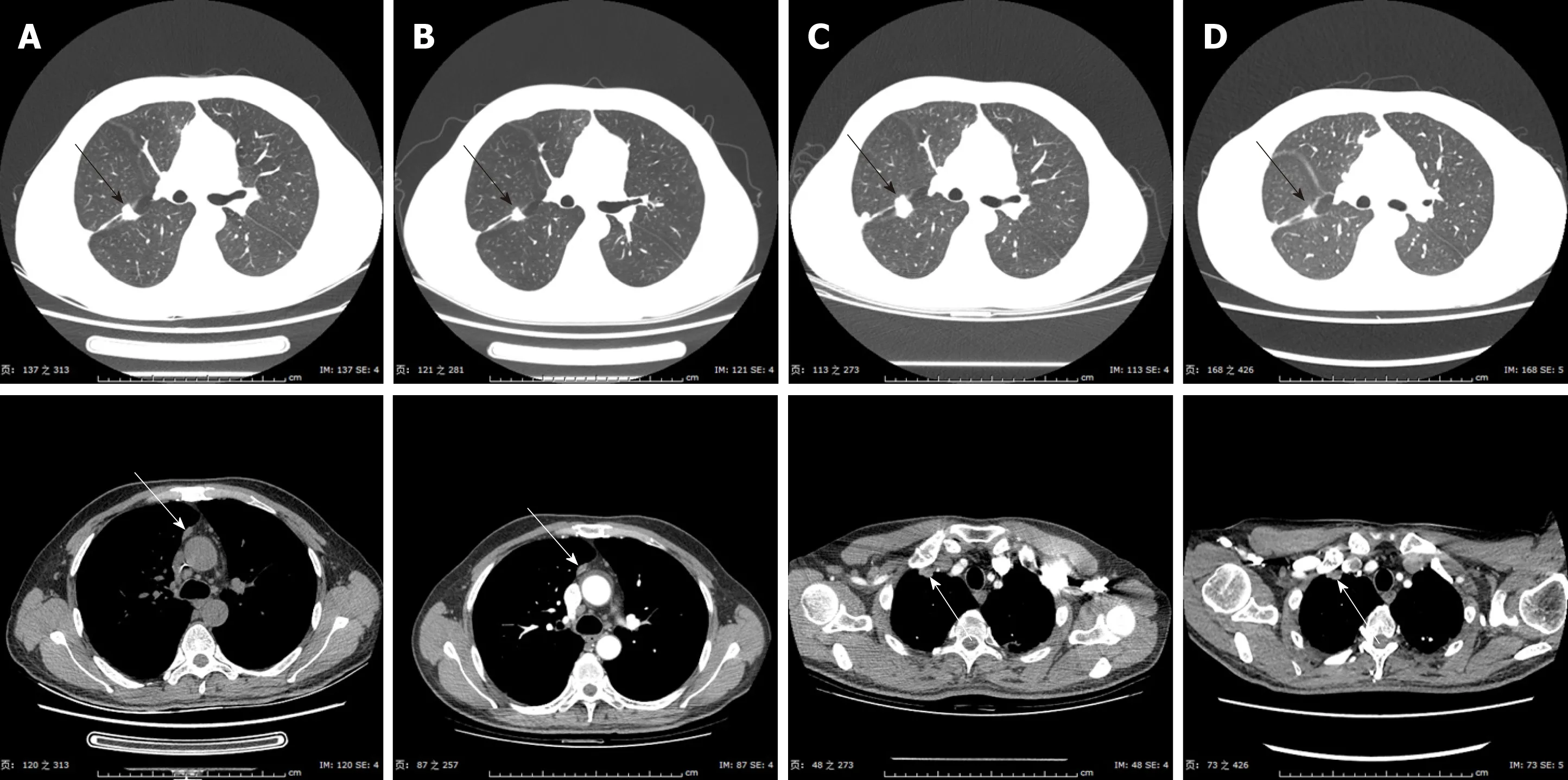
Figure4 Images from computed tomography showing the tumor response up to the fourth-line therapy of NVB + Endo.
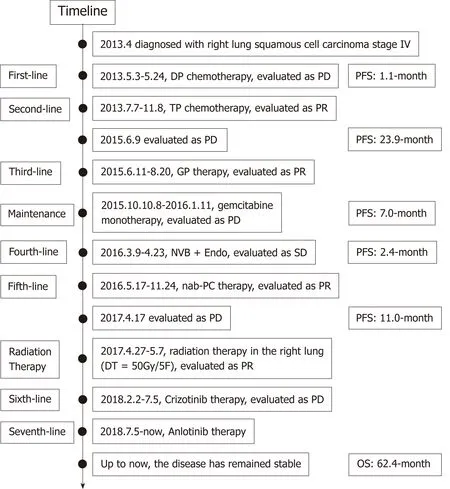
Figure5 Timeline of our case’s treatment with multiline therapy for advanced squamous cell carcinoma.
 World Journal of Clinical Cases2019年14期
World Journal of Clinical Cases2019年14期
- World Journal of Clinical Cases的其它文章
- Pulmonary Langerhans cell histiocytosis in adults:A case report
- Primary neuroendocrine tumor in the presacral region:A case report
- Noteworthy effects of a long-pulse Alexandrite laser for treatment of high-risk infantile hemangioma:A case report and literature review
- Colorectal neuroendocrine carcinoma:A case report and review of the literature
- Duodenal intussusception secondary to ampullary adenoma:A case report
- Open reduction of a total talar dislocation:A case report and review of the literature