Perioperative topical ascorbic acid for the prevention of phacoemulsification-related corneal endothelial damage:Two case reports and review of literature
2019-04-20 02:03:48ChiaYiLeeHungTaChenYiJenHsuehHungChiChenChiehChengHuangYaaJyuhnJamesMeirChaoMinChengWeiChiWu
World Journal of Clinical Cases 2019年5期
Chia-Yi Lee,Hung-Ta Chen,Yi-Jen Hsueh,Hung-Chi Chen,Chieh-Cheng Huang,Yaa-Jyuhn James Meir,Chao-Min Cheng,Wei-Chi Wu
Abstract
Key words: Ascorbic acid; Fuchs corneal endothelial dystrophy; Endotheliitis; Human corneal endothelial cell; Phacoemulsification; Case report
INTRODUCTION
Phacoemulsification has been used to treat cataract for decades,while human corneal endothelial cells (HCECs) loss remains a major complication[1].Fuchs endothelial corneal dystrophy (FECD) is a dystrophic disorder of HCECs that are vulnerable to external damage[2].Recently,corneal endotheliitis has been demonstrated to be an inflammatory process with viral origin,e.g.,cytomegalovirus (CMV),that destroys HCECs and leads to severe visual impairment[3].Because corneal decompensation with severe HCECs loss is common in patients with impaired HCECs,including corneal endothelial dystrophy,post-traumatic status and corneal endotheliitis[4,5],adequate management is advocated to prevent corneal decompensation after phacoemulsification.
Triple procedures,combining endothelial keratoplasty,phacoemulsification and intraocular lens implantation,have been successfully performed in patients with concomitant cataract and corneal decompensation[6],while limited sources of corneal donor tissues result in long waiting lists[7].Also,several complications following triple procedure have been reported,such as secondary glaucoma,graft dislocation requiring re-surgery and graft rejection leading to graft failure[8,9].We therefore wonder if there are potential strategies to prevent corneal endothelial loss other than surgical triple procedures.
Theoretically,ascorbic acid (AA) can be an ideal ocular nutritional supplement[10].Two in vitro studies have shown that AA and L-AA 2-phosphate prolonged the lifespan and inhibited apoptosis of murine corneal endothelial cells[11]and HCECs[12],probably through anti-oxidant effects.On the other hand,topical AA can be used alone to manage alkali burns which decrease the incidence of corneal ulcerations and perforation in rabbits[13],or combined with topical steroids to treat alkali burns without significant side effects[14,15].Furthermore,animal studies showed that AA applied to the irrigating solution can serve as free-radical scavengers to prevent endothelial cell damage from phacoemulsification[16,17].Still,it remains unclear whether topical AA can prevent HCECs loss after phacoemulsification.In addition,although AA has been used for protective agent of HCECs by intraoperative or postoperative administration[17-19],the perioperative instillation of AA has not been used before.
Herein,we report the use of topical AA before and after cataract surgery to reduce HCECs loss in patients with pre-existing corneal endothelial disorders.The novel effect of perioperative topical AA,which obviated the need for corneal transplantation,is demonstrated in two patients with FECD and CMV corneal endotheliitis respectively.
CASE PRESENTATION
Chief complaint
Patient 1:A 41-year-old man presented with blurry vision in the right eye.
Patient 2:A 51-year-old man was referred to our clinic due to whitish left cornea.
History of present illness
Patient 1:The symptom persisted for months without exacerbating or relieving factors.
Patient 2:The symptom persisted for 3 wk and had gradually progressed.
History of past illness
Patient 1:The patient reported no known systemic illness or previous surgery.
Patient 2:The patient revealed no known systemic illness or previous surgery.
Personal and family history
Patient 1:The patient revealed no known personal and family history.
Patient 2:The patient revealed no known personal and family history.
Physical examination
Patient 1:The best-corrected visual acuity (BCVA) in the right eye was 20/60.Slit lamp examination revealed cataract with right predominance.
Patient 2:On examination,BCVA was 20/50 in the left eye and the silt-lamp microscope revealed bilateral cataract with mild corneal edema in the left eye (Figure 1A).
Laboratory examinations
Patient 1:No laboratory examination was performed due to the absence of indication.
Patient 2:Intracameral tapping of left eye was arranged,and real-time quantitative polymerase chain reaction exam reported a positive result for CMV.
Imaging examinations
Patient 1:Specular microscopy showed bilateral guttate formations (Figure 2).
Patient 2:The specular microscope revealed ECD of 1273/mm2with disciform lesions in the left eye.
FINAL DIAGNOSIS
Patient 1:The final diagnosis of the case was bilateral cataract with right predominant and bilateral FECD.
Patient 2:The final diagnosis of the case was bilateral cataracts and CMV endotheliitis in the left eye.
TREATMENT
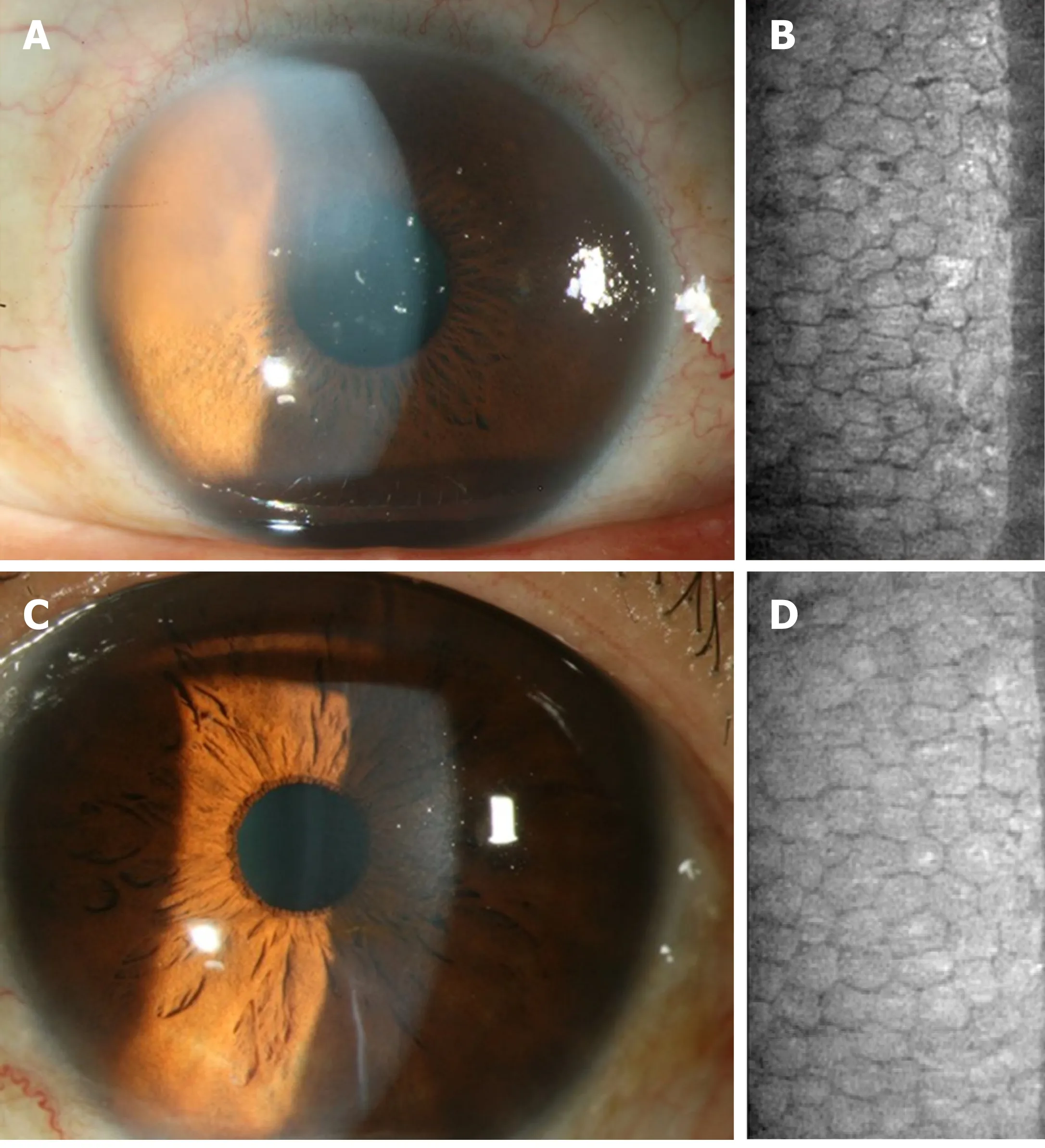
Figure 1 The corneal endothelium condition before and after cataract surgery in the left eye of Patient 2.
Patient 1:Phacoemulsification was performed,and postoperative BCVA in the right eye was 20/200; nevertheless,our patient continued to complain of blurry vision and tingling of the right eye.Specular microscopy revealed pseudophakic bullous keratopathy and Descemet's stripping.Automated endothelial keratoplasty was performed as salvage surgery.After keratoplasty,a clear cornea graft with enhanced endothelial cell density (ECD) of 2075/mm2and improved BCVA of 20/25 in the right eye were observed.Two years later,a left eye cataract was found with BCVA of 20/200 (Figure 3A) and another phacoemulsification was planned.The preoperative ECD was 1365/mm2in the left eye (Figure 3B).To prevent a similar scenario of corneal decompensation,we prescribed AA (50 mg/mL,Vitacicol,Taiwan Biotech CO.,LTD.,Taoyuan,Taiwan) eye drops four times daily one month before and after surgery.In addition,excessive intracameral medications,including lidocaine and carbachol,were avoided intraoperatively.
Patient 2:Acyclovir and famciclovir were sequentially prescribed for the suspicion of herpetic simplex virus endotheliitis; however,upper corneal edema and a few keratic precipitates emerged.Topical valganciclovir and systemic ganciclovir were prescribed for the CMV endotheliitis,and the CMV endotheliitis subsided.Meanwhile,AA (50 mg/mL) was used for the scheduled cataract surgery with a frequency of four times daily one month perioperatively.The ECD was 1048/mm2before surgery (Figure 1B).
OUTCOME AND FOLLOW-UP
Patient 1:Only mild stromal edema was observed postoperatively without bullae,while improved visual acuity was reported by the patient.The BCVA in the left eye was 20/30 with clear cornea and ECD of 1239/mm2two years postoperatively (Figure 3C and D).
Patient 2:After the surgery,the visual acuity had improved without signs of corneal decompensation.The postoperative ECD was 1017/mm2in the left eye with BCVA of 20/20 at the latest visit (Figure 1C and D).
DISCUSSION
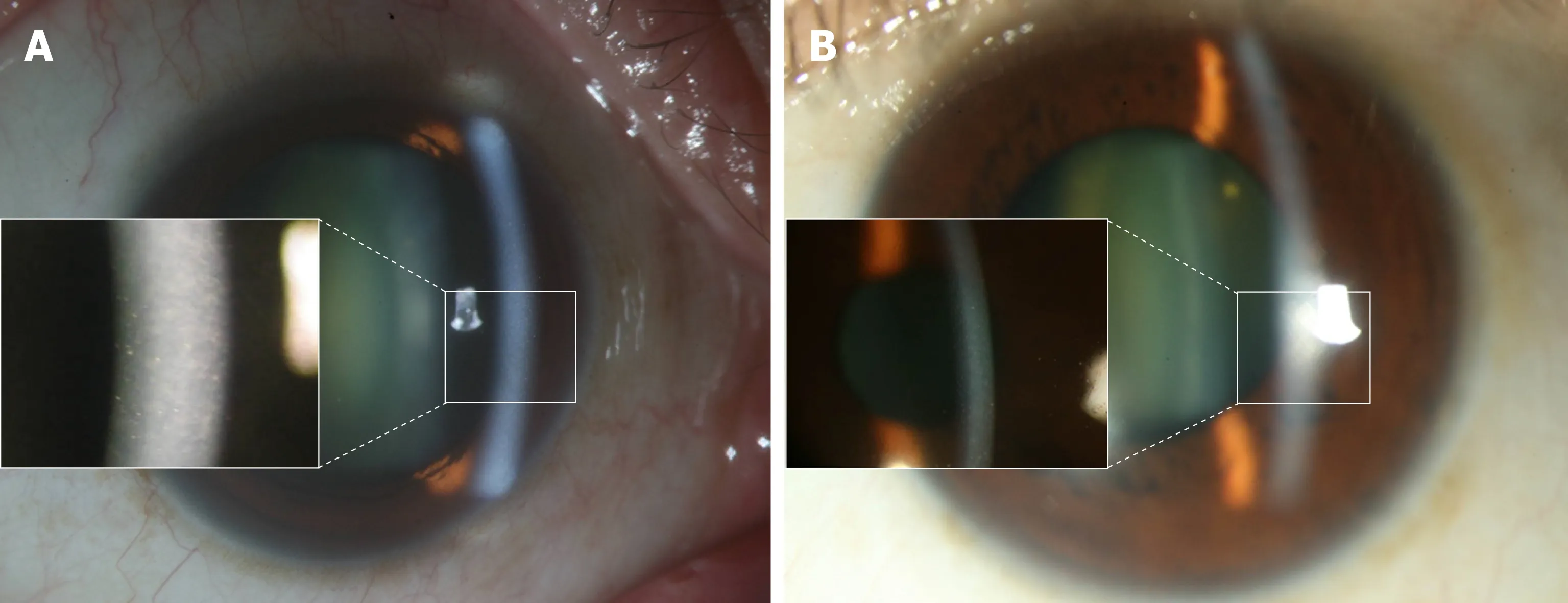
Figure 2 The appearance of Fuchs endothelial corneal dystrophy in Patient 1.
In the corneal endothelium,oxidative stress may increase lipid peroxidation,leading to cellular impairment and apoptosis of HCECs[20].FECD is featured by elevated cell apoptosis resulting from higher oxidative stress and oxygen-induced damage on DNA[20,21].Although oxidative stress has not been demonstrated in CMV corneal endotheliitis,apoptosis has been detected in CMV retinitis in cell line models[22].In addition,oxygen free radicals generated by high-intensity ultrasound oscillations in water during phacoemulsification have been shown to damage the corneal endothelium[23].Since HCECs of the two patients enrolled were impaired with ECD below 1500 cell/mm2,the double damage of phacoemulsification and concurrent FECD or CMV endotheliitis increased the risks of developing corneal decompensation or even pseudophakic bullous keratopathy.To prevent the oxidative damage,we arranged anti-oxidant therapy with topical AA and reached acceptable visual outcome with fair corneal condition.To our knowledge,this is the first experience to show the effectiveness of topical AA in the prevention of phacoemulsification-related corneal endothelial damage.
The AA has been widely applied in immune and inflammatory disorders due to its antioxidant properties recently[24].In the field of ophthalmology,previous studies illustrated that AA may be associated with the development of cataract,age-related macular degeneration and diabetic macular edema and owns the potential as a therapeutic agent[10,25-27].About the cornea,postoperatively topical instillation and oral administration of AA preserve the integrity of corneal stroma in refractive procedures[18,19],while intracameral irrigation of AA during phacoemulsification may decrease corneal endothelial injury in animal studies[17,28].Still,the effectiveness of perioperative AA instillation on the protection of HCECs demonstrated in the current study has rarely been reported elsewhere.The AA we administrated in the current study was 50 mg/mL,which was much higher than the concentration of AA in the general culture medium.However,the corneal endothelium is immersed in an environment where aqueous humor is recycled every one to two hours and the bioavailability of topical medications is only approximately one to five percent[29].As a result,we adopted a much higher concentration of AA than that of the ordinary culture medium and followed a humanly possible administration protocol of four times a day in the hope to reach similar concentration of AA in the culture medium.The favorable preservation of HCECs and absence of complications in our two patients verifies the current concentration of AA as acceptable whether in terms of efficacy or safety.
The first patient was diagnosed with FECD.In a previous study,35 of 89 eyes needed to undergo endothelial keratoplasty,but no improvement in BCVA was found in those eyes that underwent endothelial keratoplasty[6].By comparison,BCVA in the left eye of the first patient recovered prominently.Our findings suggest that perioperative anti-oxidant supplements can improve and preserve HCECs and visual outcomes compatible with the degree of the traditional approach.Furthermore,graft dislocation and pupillary block glaucoma occasionally occur in patients undergoing triple surgery despite excellent visual outcome[30],while current management avoids these complications.
For patients with corneal endotheliitis who require cataract surgery,previous studies focused only on postoperative infection[31],or did not provide adequate details regarding postoperative status[5].In the current study,the second patient was diagnosed with CMV endotheliitis and low ECD,while the final BCVA was 20/20,showing much improvement with similar ECD values observed postoperatively.A possible explanation is that phacoemulsification-related oxidative stress can be alleviated by AA and that the anti-inflammatory effect of AA may also reduce the inflammation from both phacoemulsification and CMV endotheliitis[32].
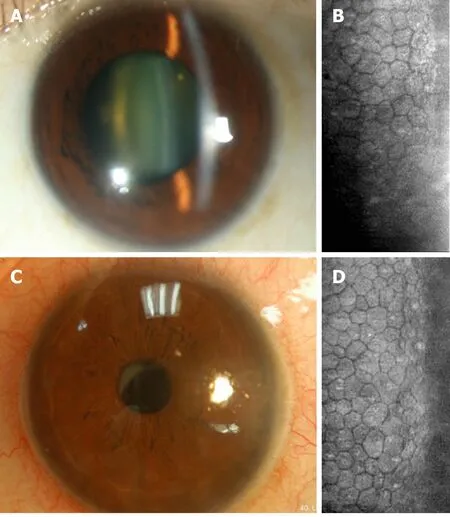
Figure 3 The corneal endothelium condition before and after cataract surgery in the left eye of Patient 1.
Comparison of the current study to two previous studies concerning the application of phacoemulsification in low ECD patients is illustrated in Table 1.The two previous studies applied a soft-shell technique to reduce possible mechanical impact[4,5].We did not perform the soft-shell technique but rather used an ophthalmic Viscoat viscoelastic device and irrigation with balanced salt solution.Furthermore,we did not alter the perioperative medications except AA among all eyes undergoing cataract surgery mentioned in this report.Collectively,the use of perioperative topical AA alone ended up with similar HCECs loss compared to previous experiences[4,5].Moreover,the major etiology of low ECD in a previous study was primary angle closure glaucoma with acute attack or laser iridotomy[4],possibly inducing less damage to HCECs than HCECs-origin lesions such as FECD.
CONCLUSION
Perioperative topical AA showed both safety and promise for prevention of HCECs dysfunction in high-risk patients undergoing phacoemulsification and may be considered an alternative therapy.Further large prospective studies are required to determine the optimal dose.
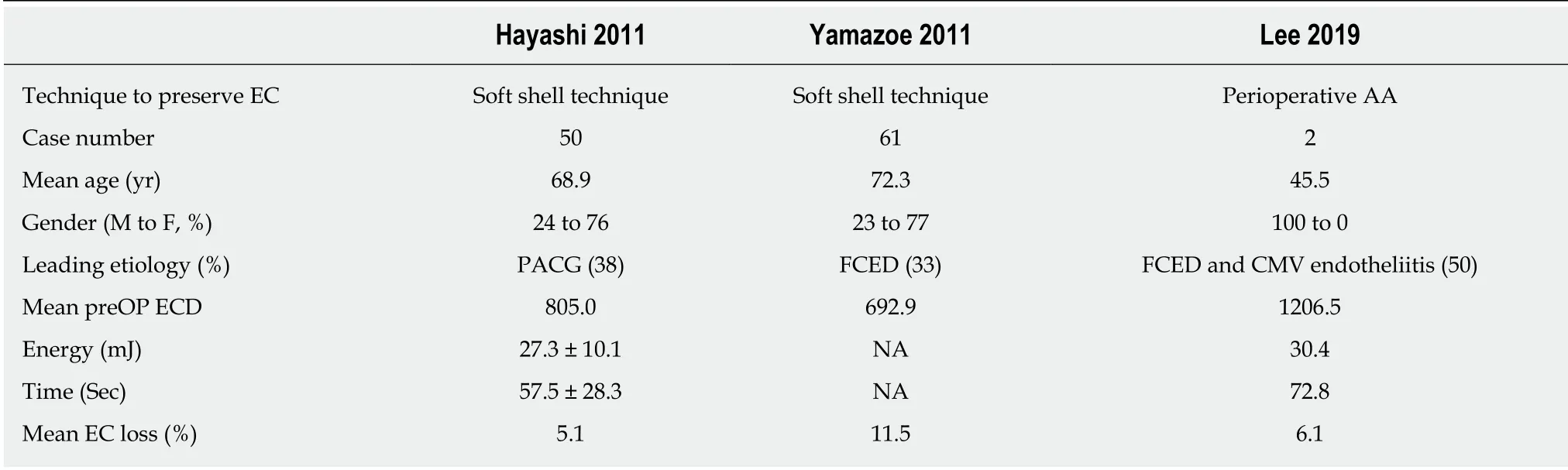
Table 1 Comparison of different modifications of cataract surgery in patients with low endothelial count
 World Journal of Clinical Cases2019年5期
World Journal of Clinical Cases2019年5期
- World Journal of Clinical Cases的其它文章
- Melanotic Xp11-associated tumor of the sigmoid colon:A case report
- Intrauterine cystic adenomyosis:Report of two cases
- Use of tunnel endoscopy for diagnosis of obscure submucosal esophageal adenocarcinoma:A case report and review of the literature with emphasis on causes of esophageal stenosis
- Rare empty sella syndrome found after postoperative hypotension and respiratory failure:A case report
- Concomitant paraganglioma and thyroid carcinoma:A case report
- Application of computer-assisted navigation in treating congenital maxillomandibular syngnathia:A case report