Non-lnvasive management of invasive cervical resorption associated with periodontal pocket:A case report
2019-04-16 08:21:04AbdullahAlqedairi
World Journal of Clinical Cases 2019年7期
Abdullah Alqedairi
Abstract
Key words: Invasive cervical resorption;Mineral trioxide aggregate;Non-surgical root canal;Periodontal;Case report
INTRODUCTION
Invasive cervical resorption (ICR) denotes a particularly aggressive form of external tooth resorption that progressively destroys the tooth structure within the dentition[1,2].This clinical condition serves the purpose of progressively destroying the tooth structure within the dentition.It is notable due to its position with regards to the cervical region of the tooth and its invasive properties and can be visualized as a pinkish color in the crown of the tooth[2].This color occurs due to coronal dentin and enamel resorption,due to which the intensely vascular resorptive tissue can be visualized through the residual enamel[3].A clinical classification of ICR has been proposed by Heithersay based on the extension of dentin destruction[2].Class 1 demonstrates a small invasive resorption near the cervical area with shallow penetration into dentin.Class 2 demonstrates a well-defined,close to the coronal portion of the pulp cavity with little or no extension to the root dentin.Class 3 represents a deeper invasion of dentine by resorbtive defect and extending into the coronal third of the root.Class 4 corresponds to a large invasive resorption extending beyond the coronal third of the root[2].
Numerous complications surround the effective and accurate diagnosis of ICR primarily due to its consistent misinterpretation as a form of internal resorption[3].Research indicates a lack of clarity surrounding the etiology of this condition.Moreover,various factors may predispose an individual to ICR.Literature noted that the primary contributing factor was intra-coronal bleaching,followed by orthodontics,trauma and other dentoalveolar surgery periodontal treatments[4].
健美操動作多樣且動作與動作之間可以靈活的組合,使之具有很高的觀賞性,給予人健美操的特有的美感。而且健美操動作中不僅包含基本的動作,也包含高難度動作,這就需要提供安全且完善的場地設備,以保證教師與學生的安全,避免不必要的危險和傷害發生。因此河南省高校健美操課程場地設施的缺乏也是影響河南省高校健美操課程持續發展的重要因素。
ICR affects the periodontal tissues within the dentition and this clinical condition is considered as one of the primary factors due to which periodontal tissue inflammation may arise[5].However,ICR does not have any pulpal interaction,since the pulp is shielded by a predentin layer.Studies indicate the role of bacterial involvement in the gingival sulcus in sustaining the inflammation within the periodontal tissues[6-8].Moreover,the occurrence of ICR was found to be extremely prevalent below the tooth’s epithelial attachment.Therefore,it is of great significance to take into consideration the fact that the location of ICR is not always cervical.This is because,the location is associated with the level of marginal tissues and the depth of the periodontal pockets[9].It is critical that resorption be terminated via the utilization of suitable dental treatment.The present case study discusses the utilization of non-surgical root canal treatment in conjunction with mineral trioxide aggregate (MTA) to form the treatment of a patient with ICR associated with Periodontal Pocket.
CASE PRESENTATION
Chief complaints
A 21-year-old female patient presented to endodontic clinic at the University Dental Hospital at King Saud Dental University with the chief complaint of intermittent spontaneous pain related to upper left side.
History of present illness
Patient has recently noticed a small localized swelling between teeth in the maxillary left posterior region.The pain started at the same area a month ago.Patient reported no sensitivity to cold or heat stimulation.
History of past illness
The patient reported no history of trauma.However,she had received orthodontic treatment 2 years ago.The patient had multiple restorations mostly carried out by a pedodontist one year prior to her admittance at this hospital.
Personal and family history
Patient medical history was noted to be noncontributory.
Physical examination upon admission
Clinical examination revealed the presence of localized erythematous swelling at the buccal interdental papilla between the left maxillary first molar and second premolars(Figure 1A and B).
It was noted that the left maxillary second premolar and first molar had MOD tooth-colored restorations.Meanwhile,the left maxillary second molar had MO amalgam restorations.The teeth were tested electrically and thermally.It was found that left maxillary first molar was not responsive to the thermal or electric pulp tests;whereas,the other tested teeth responded normally.Moreover,it was noted that this tooth was sensitive to percussion and tender to palpation.On probing,a respective pocket depth of 12 mm and 10 mm was detected in the mesiobuccal and mesiolingual regions of left maxillary first molar (Figure 1C and D).
Imaging examinations
A two-dimensional radiographic examination was conducted that revealed the presence of a breakdown of the crest of alveolar bone mesial to left maxillary first molar and an irregular molted radiolucency mesial to the pulp space of left maxillary first molar but separated by radiopaque line,and extending into the radicular dentin(Figure 2A and B).Cone-beam computed tomography examination confirmed the size and the external perforation of the existing resorption defect (Figure 2C).
FINAL DIAGNOSIS
Based on the clinical and radiographic findings,the left maxillary first molar was diagnosed as necrotic pulp with symptomatic apical periodontitis.Furthermore,the resorptive lesion was diagnosed as a perforating class 3 grade of ICR that was associated with secondary periodental disease.
TREATMENT
A treatment plan was presented to the patient that was inclusive of nonsurgical root canal therapy and the repair of the resorptive defect via an orthograde approach using white MTA.A questionable prognosis was considered due to the extension and location of the resorptive defect.Consent was obtained from the patient.The first treatment session incorporated the administration of local infiltration anesthesia and tooth isolationviarubber dam.Upon access cavity preparation,excessive bleeding was noted at the anticipated location of resorption defect.The defect was temporarily sealed with Oraseal (Ultradent Products Inc.,South Jordan,Utah the United States)and complete access was performed.Mesiobuccal,distobuccal and palatal canals were located and negotiated to the full length,and their patency was established using a size 10 k-file (Dentsply/Maillefer,Ballaigues,Switzerland).
Following this,a chemo-mechanical preparation using a profile rotary system(Maillefer,Ballaigues,Switzerland) was carried out.Mesiobuccal and distobuccal canals were prepared to size 35/04,while the palatal canal was prepared to dimensions of 40/06.The preparation of the canals was consistently carried out under irrigation using 5.25% sodium-hypochlorite solution.Subsequently,the resorption defect was exposed and the granulomatous tissue was removed using a spoon excavator instrument and a size 2 round carbide bur (Komet Dental,Lemgo,Germany).Two small perforations and the second mesiobuccal canal were located at the base of the resorptive defect.It is to be noted that the visibility was compromised due to the excessive bleeding.Therefore,the root canal system and the resorption defect were dressed with calcium hydroxide (Ultradent Products Inc.,South Jordan,Utah the United States) and the tooth was then provisionally restored using cotton and cavit (coltene,Alstatten,Switzerland).One week later,the patient presented to the clinic and was found to be asymptomatic.The tooth was reopened and calcium hydroxide was removed.The bleeding due to the resorption defect was controlled and better visibility was achieved (Figure 3A and B).The second mesiobuccal canal was negotiated and prepared to size 30/04.The mesiobuccal root demonstrated type II root canal configuration according to the Vertucci classifications[10].
The canals were later irrigated using 17% EDTA (SybronEndo,Orange,Ca).Furthermore,5.25% NaOCL was used as final rinse for the canals.Obturation of the root canal system was performed using the continuous wave of vertical condensation technique through the use of gutta percha and AH26 (Dentsply,Konstanz,Germany)(Figure 3C).The resorption defect and the two mesiobuccal canals orifices were sealed with white MTA (Dentsply/Maillefer,Ballagiues,Switzerland) (Figure 3D).The tooth was then provisionally restored with wet cotton and cavit.The postoperative radiograph revealed that there was adequate MTA filling of the perforation and resorption defect (Figure 4).One week later,the tooth was reopened,the setting of MTA was confirmed and the tooth was restored with bonded restoration using a multicore medium (Ivoclar Vivadent,Schaan,Liechtensien).Subsequently,the tooth was prepared and an impression was taken for the coronal overlay.

Figure 1 Clinical findings.
OUTCOME AND FOLLOW-UP
Two weeks later,clinical examination revealed the presence of normal color in the surrounding soft tissue and a normal response to percussion and palpation.Probing depths around the tooth were within normal limits (3-4 mm) and the epithelium attachment was regained.At the one-year recall,the tooth showed no symptoms and responded normally to percussion and palpation.It was noted that the surrounding periodontium exhibited a normal color and the probing depth was likewise noted to be normal.The radiographic examination showed a restoration of the crestal alveolar bone and good adaption to the MTA (Figure 5).Figure 6 represents the timeline from the patient’s presentation to the final outcome.
DISCUSSION
The case study has explored the efficacy of non-surgical approaches to treat ICR.A patient reporting intermittent pain at the upper left side,no history of trauma,with multiple restorations and having received orthodontic treatment previously was studied.It was noted that orthodontic treatment and restorations were the predisposing factors that heavily contribute to the development of ICR[4].A non-surgical approach in the form of root canal treatment and orthograde repairviaMTA was utilized to effectively manage ICR in the patient.
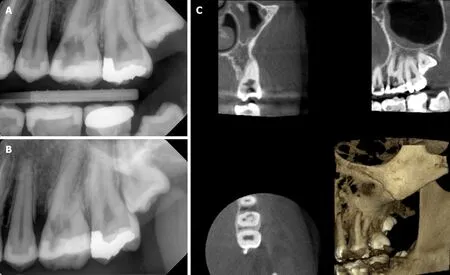
Figure 2 Radiographic findings.
In the recent years,studies have highlighted the efficacy of non-surgical approaches in the effective management of ICR,associated with the periodontal tissues.It was noted that such non-surgical approaches combine root canal treatment with orthograde repair of the region,where there is the presence of resorptive defect[11].Such studies conducted a removal of diseased tissue and orthograde repair via the use of materials;such as MTA,as in the present case study.Studies reported that this material demonstrated good sealing ability that can serve as repair material for perforations[12,13],and has excellent biocompatibility[7].
The use of MTA with regard to orthograde repair and as an obturation material was noted to be extremely advantageous in studies that discussed its applications as a hermetic seal in root end filling[9].More recently,new bioceramic formulations,such as Biodentin,EndoSequence?BC Sealer?,Root Repair Material (RRM?),and Fast Set Putty (Brasseler the United States?),have been introduced as an alternative to MTA,due to their better physical,chemical,and biological properties,and to overcome the drawbacks associated with the use of MTA like handling properties,long setting time and tooth discoloration[14-17].This study additionally incorporated the use of EDTA and NaOCl to irrigate and rinse the canals.This use of EDTA and NaOCl was further noted in additional studies that have conducted reviews of non-surgical management of ICR[10].
As discussed earlier,the results depicted that the use of non-surgical treatment aided in the normalization of response to percussion and palpation,as well as the normalization of color in the surrounding soft tissue.It was further seen that the probing depths around the tooth were normal,and the epithelial attachment was recovered.The normal color and response to percussion and palpation was further noted at the one-year recall.Furthermore,the probing depth was noted to be within the normal limits,and the surrounding periodontum was seen to be normal in color.This normal probing depth after non-surgical managementviaMTA was noted in other studies that conducted a 1-year follow up after the treatment[6].Additionally,the radiographic examination depicted restoration of crestal alveolar bone and good adaption to MTA (Figure 5).The use of radiographic analysis to assess the level of ICR was highlighted by Heithersay.This restoration of the crestal bone was further noted in additional studies that conducted examinations of the effective management of ICR[8].
CONCLUSION
ICR is an uncommon type of tooth resorption that is commonly misdiagnosed as a form of internal resorption.This condition may further impact the periodontal tissues that result in the development of deep periodontal pockets.Non-surgical management of ICR was discussed in various studies as an effective way of managing this condition.This study made use of root canal treatment and orthograde repair via MTA to manage ICR.At two weeks and one-year follow-ups,normalcy with respect to color,probing depth,response to percussion,and palpation was recovered.Furthermore,the crystal alveolar bone structure was also restored.These results are in support of the effective role of non-surgical approaches in the management of ICR.It is recommended that early diagnoses should be carried out with regards to ICR;so that non-surgical approaches may be utilized instead of surgical interventions.Furthermore,it is highly recommended to make use of MTA as a sealing material in orthograde repair due to its excellent sealing capabilities and biocompatibility.
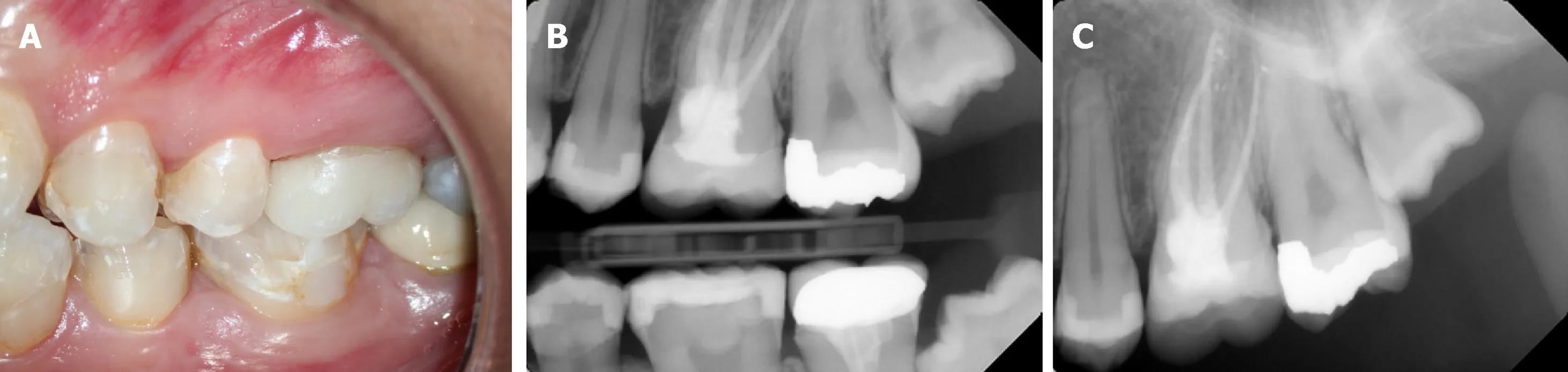
Figure 5 One-year recall:Probing depths around the tooth within normal limits of 3-4 mm and restoration of the epithelial attachment and crestal bone.

Figure 6 Timeline summarizing the patient’s information,clinical findings,diagnostic tests,diagnosis,intervention,and follow up.
ACKNOWLEDGEMENTS
The author thanks King Saud University,College of Dentistry Research Center(CDRC No.FR 0430) for their assistance in conducting this study.
猜你喜歡
快樂語文(2021年27期)2021-11-24 01:29:04
內蒙古教育(2021年20期)2021-03-08 01:09:14
計算機教育(2020年5期)2020-07-24 08:53:38
甘肅教育(2020年22期)2020-04-13 08:11:16
家庭影院技術(2019年11期)2019-12-09 09:14:30
福建基礎教育研究(2019年3期)2019-05-28 23:14:43
小學生作文(低年級適用)(2018年3期)2018-04-17 00:58:35
少年博覽·小學低年級(2017年4期)2017-06-09 16:22:28
作文評點報·低幼版(2017年7期)2017-03-11 20:49:41
少兒科學周刊·少年版(2015年4期)2015-07-07 20:56:37
 World Journal of Clinical Cases2019年7期
World Journal of Clinical Cases2019年7期
- World Journal of Clinical Cases的其它文章
- Type l congenital extrahepatic portosystemic shunt treated by orthotopic liver transplantation:A case report
- Min-invasive surgical treatment for multiple axis fractures:A case report
- Villous adenoma coexistent with focal well-differentiated adenocarcinoma of female urethral orifice:A case report and review of literature
- Congenital bronchobiliary fistula:A case report and review of the literature
- Robot-assisted gallbladder-preserving hepatectomy for treating S5 hepatoblastoma in a child:A case report and review of the literature
- Vein of Galen aneurismal malformations - clinical characteristics,treatment and presentation:Three cases report