OxyContin and the McDonaldization of chronic pain therapy in the USA
2019-04-11 06:27:34JordanHughesNeelimaKalePhilipDay
Jordan Hughes, Neelima Kale, Philip Day
ABSTRACT Principles and practices gleaned from successful business enterprises have been used to transform the practice of medicine for decades. McDonaldization is the process in which principles which govern fast-food businesses, are applied to the practice of medicine. When left unchecked,the application of these principles can have devastating consequences, as in the treatment of chronic, nonmalignant pain with OxyContin. At a time when there was growing concern about the under treatment of pain,Purdue Pharma introduced OxyContin, providing an efficient, predictable way of treating chronic pain. The liberal prescription of this drug contributed, and continues to contribute, to the opioid epidemic we see today. So, in confronting this epidemic, we must first understand the process of McDonaldization that has brought us here and then provide safe and effective chronic pain therapies even if they are expensive, time-consuming to deliver, dif fi cult to measure, and unpredictable in their outcomes-all things we’ve grown to detest in our McDonaldized healthcare system.
Twenty-five years ago, sociologist George Ritzer expressed his concern for the ways in which American society was being transformed by the principles that govern fast-food businesses—a process he termed McDonaldization.1This fast-food model involves taking efficiency, calculability, predictability and control to their extremes in order to produce a streamlined, profitable business(see table 1). While acknowledging the obvious benefits of these principles, Ritzer warned that the extremes of their implementation result in serious, often-overlooked consequences. We use this framework below to understand the history of chronic, non-malignant pain treatment in the USA and how the McDonaldization of American society has contributed to the present opioid crisis. Additionally, throughout this analysis, OxyContin,and its manufacturer Purdue Pharma, will be used as an example of how the advertisement of opioid analgesics was so effective and advanced the McDonaldization of chronic pain therapy.
In the early 1990s, the medical community became increasingly concerned with the widespread undertreatment of pain. Addressing this issue, the President of the American Pain Society told his members that physicians should begin to ‘treat pain as a vital sign’.2This directive set in motion a national effort to put a greater emphasis on pain management,including the Joint Commission requiring hospitals to ‘recognize the right of individuals to receive appropriate assessment and management of pain’ and ‘incorporate pain management into the organization’s performance measurement,’ using a 10-point Likert scale as the principle measure of pain.3While a noble effort given the staggering number of Americans living with chronic pain, many front-line providers around the country did not have the requisite training to treat pain safely and effectively.
Many physicians were already facing the demands of the McDonaldization of medicine, such as being efficient in their patient visits, meeting metrics of productivity and complying with myriad billing regulations.4So with this new emphasis on pain management and a mandate to prioritise it, physicians were confronted with greater responsibility without any new tools to help meet the challenge.56
Enter OxyContin…
This was the miracle drug to cure the woes of the patient in pain, as it was so aggressively advertised, and those of the physician.7The McDonaldization of medicine was increasing the demands of physicians, and OxyContin provided relief from many of the difficulties associated with treating some of the most challenging and time-consuming patients—those with chronic, non-malignant pain. From the busy physician’s perspective, this was a drug with powerful, long-lasting analgesic qualities and a claimed less than 1% addiction rate, so there was little motivation to consider non-pharmacological or non-opiate therapies.7After all, OxyContin was promoted as the drug ‘to start with and to stay with’.8And thus, the McDonaldization of chronic pain therapy began contributing to what would soon be an epidemic.
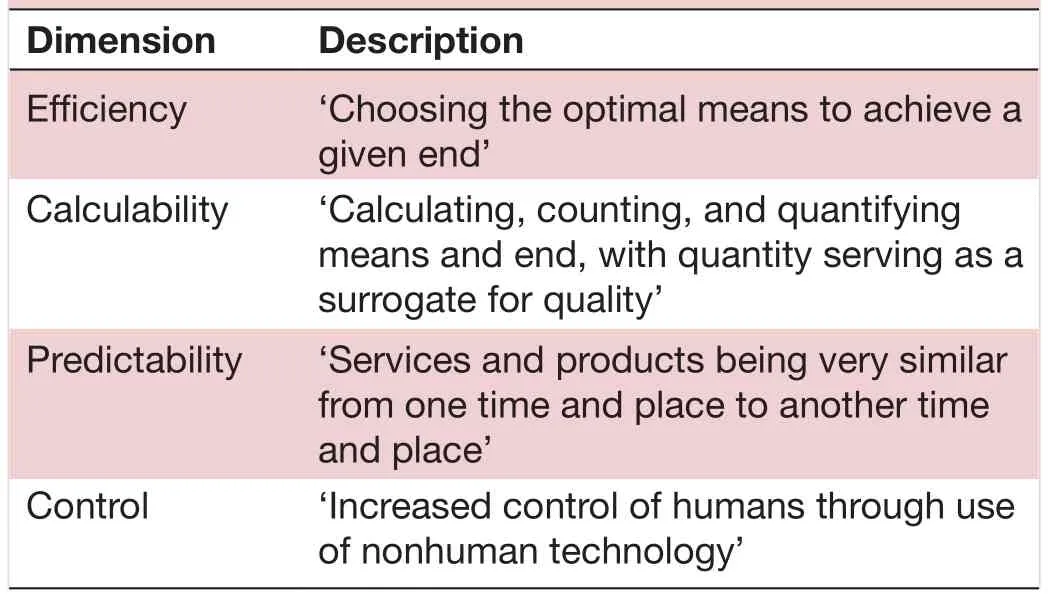
Table 1 Dimensions of McDonaldization4
The first dimension of McDonaldization, efficiency, is something physicians were already very familiar with,as healthcare delivery became increasingly driven by the demands of the bottom line. Just as McDonald’s employees are taught to swiftly and methodically churn out hamburgers for their hungry customers, physicians were expected to treat more patients in a shorter amount of time—a goal for which the slow, attentive evaluation and therapy patients in pain require are not amenable.But with the release of OxyContin, physicians could bring patients in pain into the fold of efficiency, simply writing them a prescription for the drug and giving instructions to call if the pain was not controlled, so they could issue a higher dose.8
Calculability—the second dimension of McDonaldization—focuses on the quantity of goods and services delivered, and is arguably the largest contributor to the opioid crisis we face today. With the undertreatment of pain a recognised issue, what simpler, cleaner indication of positive progress in this area than a substantial increase in analgesic prescriptions? Besides, insurance companies were far more likely to cover a prescription for OxyContin than time with a social worker or in talk therapy. And with the pain Likert scale being used to judge quality of care,physicians only stood to gain from prescribing more of the powerful analgesic. Thus, OxyContin prescriptions rose ‘from about 670 000 in 1997 to about 6.2 million in 2002’.8So, much like McDonald’s, which on its signs boasts the billions of hamburgers it has sold, the medical community was relying on the number of prescriptions of OxyContin being written to help measure its success in treating pain. But as Dorsey and Ritzer point out, ‘quantity is often a poor surrogate for quality’.4While more patients were being treated and profits were climbing, addiction to the drug was reaching epidemic proportions.7
The third dimension of McDonaldization, predictability,is critical for the fast-food chain, so it can ensure consistent food quality, employee productivity, customer experience, and so on. But when applied to the treatment of chronic pain with OxyContin, there were devastating consequences. These resulted in part because pain,inherently subjective and multiform, was now being treated as a vital sign—the rest of which are precise,objective measures. With drugs to predictably treat issues involving the other vital signs, physicians needed drugs to do the same for pain. OxyContin provided that effective,uniform treatment, which led to increased predictability for both patients and physicians. This was a welcome option, as the efficacy of alternative pain therapies varied widely and often left patients feeling dissatisfied and frustrated with their continued suffering.
The fourth dimension of McDonaldization is control—control of employees, of the system and of consumers.McDonald’s uses a controlled system, comprising a combination of humans, computers and cooking technologies to serve ‘precut and preprepared food’ to hungry customers, eager for their salty fix.4This system minimises the need for human creativity and effort on the part of both employee and consumer. In the context of chronic pain management, OxyContin worked very similarly and thus produced a strange control over both doctor and patient. Physicians no longer had to parse out what exactly the cause(s) of a patient’s pain was and what therapies they might benefit from, but rather, now had the option of giving one drug to keep it all at bay. Purdue Pharma’s aggressive and patently false advertising of the safety of the drug positioned OxyContin as the most rational and efficient choice a physician could make in treating a patient in pain. This only served to benefit the controlled McDonaldized system Purdue Pharma was helping construct, because people—physicians included—are‘the great source of uncertainty, unpredictability and inefficiency in any rationalizing system’.1Furthermore,it requires no persuasion to say that OxyContin also had control over its consumers—patients. The addictive nature of the drug and the body’s ability to develop tolerance to it kept patients coming back for more and more pills in higher and higher doses.8
The realisation of what opioids have done to the McDonaldization of chronic pain therapy is felt by all physicians, but most notably the primary care doctor.The responsibility of treating patients with chronic pain often falls to primary care physicians, and as such,they were Purdue Pharma’s prime target in expanding the ‘OxyContin prescribing base’.8With the increasing demands of medical McDonaldization, one of the highest burnout rates of all physician specialties, and the shortage of primary care physicians ever growing, they were understandably susceptible to believing the promises of the drug.9Furthermore, these physicians were already fighting multiple American epidemics, like pre-diabetes and hypertension (for which McDonald’s itself happens to be a significant contributor). So, if there was a quick,effective treatment for another complex finding—pain—available, then there was little desire or opportunity to take the time to question the legitimacy of Purdue’s claims. Thus, they prescribed the drugs liberally, as they were instructed to at their Purdue-funded educational conferences.7
Now, without diminishing the utter lack of ethical concern pharmaceutical companies like Purdue Pharma displayed, it is important to emphasise that the McDonaldization of pain management had already begun before the height of Purdue’s aggressive marketing of OxyContin.7With reliance on a subjective Likert scale for pain evaluation and that same scale being used to judge physician performance, chronic pain management was becoming a business based on pleasing the customer in the short term, rather than on concern for long-term health.3Additionally, by way of coverage and reimbursement disparities, insurance companies had already limited access to other aspects of chronic pain therapy,namely mental health services.10This resulted in opioid analgesics like OxyContin often being the most economical (and therefore realistic) option for effective pain management. By continuing to McDonaldize, the healthcare system opened the door for Purdue Pharma to take advantage of the changing landscape and maximise those changes in pain management.
This is not all to say that the dimensions of McDonaldization—efficiency, calculability, predictability and control—are in and of themselves defective and/or detrimental to a system. But rather, when companies who are more accountable to investors than the Hippocratic Oath are allowed to influence clinical practice and patients’lives to the degree that Purdue did, there is considerable risk of causing patients harm, and even developing mass epidemics. We want to benefit from the good the dimensions of McDonaldization bring, but do so cautiously so as not to let them supersede our care and humanity. We want to build efficient, calculable, predictable and controlled methods of caring for our patients, with the bottom line serving as just one of many measures of success. But until that day, we face a unique challenge in chronic pain management: de-McDonaldization.
We have to take a step back and provide care that, for now, is time consuming, inefficient, less predictable and less profitable, and we must manage our patients’ expectations. Many of our patients (and ourselves, if we are honest) have become accustomed to, and comfortable in,a society that rewards businesses that have McDonaldized.We want what we want when we want it, and we often do not want to take full responsibility for what is ours to care for, including our pain. We want a pill for chronic pain relief, not a diet and lifestyle change—a steak at a McDonald’s price.
Yes, alternative pain therapies can feel inefficient, with results that are difficult to predict and control. But this is the direction we need to head in. It is a radical adjustment for many patients and physicians, but one we must undergo to become better physicians, healthier people and a stronger society that values quality over expediency and sustainability over immediacy. Otherwise, we will move closer and closer to a form of drive-thru medicine—an absurd yet conceivable future.
AcknowledgementsThe authors acknowledge the support of the Department of Family and Community Medicine at the University of Texas Southwestern Medical School.
ContributorsJH, NK and PD contributed to the conceptualisation, drafting,reviewing, editing, revising and final approval of the content.
FundingThe authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interestsNone declared.
Patient consent for publicationNot required.
Ethics approvalThe content presented in this article is not regulated human subjects research and does not require approval by an Institutional Review Board(IRB).
Provenance and peer reviewNot commissioned; internally peer reviewed.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4.0
 Family Medicine and Community Health2019年1期
Family Medicine and Community Health2019年1期
- Family Medicine and Community Health的其它文章
- Lack of validity of self-reported mammography data
- Obstacles for Iranian rural population to participate in health education programmes: a qualitative study
- Qualitative study to identify the perception and challenges faced by the faculty of community medicine in the implementation of competency-based medical education for postgraduate students
- Health services utilisation and responsiveness profiles in Iran: a provincial household study
- Out-of-pocket expenditure of families on the healthcare of children younger than 5 years
- Journey of a Lifetime