產婦產褥期尿失禁情況及其治療意愿調查
2019-01-22 04:36:08王巧紅張俊清
中國醫學創新 2019年29期
王巧紅 張俊清
【摘要】 目的:了解產婦產褥期尿失禁(urinary incontinence,UI)的發生情況以及產婦對UI治療意愿的現狀和影響因素。方法:以2017年7-12月在本院復查的1 182例產后6~8周的產婦為調查對象,采用國際尿失禁咨詢委員會尿失禁問卷簡表(ICIQ-SF)調查產婦產褥期UI發生情況,對UI產婦進一步調查其治療意愿情況。結果:產褥期UI發生率17.68%(209/1 182),以壓力性尿失禁(SUI)為主,占76.08%(159/209),其中64.11%(134/209)為輕度,30.14%(63/209)為中度,僅5.74%(12/209)為重度。在UI產婦中,60.29%(126/209)有治療意愿,且UI嚴重程度及產婦的文化程度與產婦治療意愿有關(P<0.05)。結論:產婦產褥期UI發生率較高,治療意愿不強,有必要開展產后UI的早期篩查,同時進一步提高產婦對UI的認知及重視程度,探索適合產后UI臨床特點及產婦需求的防治策略。
【關鍵詞】 產婦 產褥期 尿失禁 治療意愿
Investigaton on Prevalence of Urinary Incontinence in Puerperium and Treatment Willingness of Parturients/WANG Qiaohong, ZHANG Junqing. //Medical Innovation of China, 2019, 16(29): -160
[Abstract] Objective: To investigate the occurrence of urinary incontinence(UI) in puerperium of parturients, status quo and influencing factors of UI treatment willingness. Method: From July to December 2017, 1 182 parturients re-examined in our hospital at 6-8 weeks postpartum were selected as subjects. The occurrence of UI in puerperium of parturients were investigated by the international consultation on incontinence questionnaire short form (ICIQ-SF). And the treatment willingness of UI parturients were further investigated. Result: The incidence of UI in puerperal period was 17.68% (209/1 182), with stress incontinence (SUI) dominated, accounting for 76.08% (159/209), of which 64.11% (134/209) was mild, 30.14% (63/209) was moderate, and only 5.74% (12/209) was severe. Among UI parturients, 60.29% (126/209) had treatment willingness, and the severity of UI and education were related to the treatment willingness of parturients (P<0.05). Conclusion: The incidence of UI in puerperal is high and the treatment willingness is not strong, so it is necessary to carry out early screening of postpartum UI, further improve the awareness and attention of postpartum UI, and explore prevention and treatment strategies suitable for postpartum UI clinical characteristics and maternal needs.
[Key words] Parturient Puerperium Urinary incontinence Treatment willingness
First-authors address: Peoples Hospital of Beijing Daxing District, Beijing 102600, China
doi:10.3969/j.issn.1674-4985.2019.29.041
尿失禁(urinary incontinence,UI)是一種最常見的盆底功能障礙性疾病,嚴重影響了女性的身心健康及生活質量[1],近3成左右的成年女性受UI的困擾[2]。盡管如此,據研究報道,大多數UI患者并未因UI就醫,普遍存在診斷與治療的延遲[3-5]。有研究表明,產褥期UI與遠期UI的發生密切相關[6-7],因此,對產后UI早期的篩查診斷及干預非常有必要。本研究旨在調查產婦產褥期UI的發生情況以及臨床特點,并了解UI產婦的治療意愿及其影響因素,從而為臨床開展有針對性的UI防治策略提供依據。
1 資料與方法
1.1 一般資料 以2017年7-12月在本院門診產后復查的產婦為調查對象。納入標準:能正常溝通交流者。排除標準:(1)有盆腔大手術史者;(2)合并嚴重內外科疾病者;(3)生殖、泌尿系感染者;(4)有精神疾病病史者。所有產婦及家屬均知情同意并簽署知情同意書。本研究已經北京市大興區人民醫院醫學倫理委員會審核批準。
1.2 方法 本研究采用問卷調查法,問卷包括三部分。(1)一般資料,包括產婦的年齡、產后BMI、文化程度、產次、家庭月收入;(2)國際尿失禁咨詢委員會尿失禁問卷簡表(the international consultation on incontinence questionnaire short form,ICIQ-SF)。此量表信效度良好,用來篩查UI、評估UI的嚴重程度和對患者生活質量的影響。共有4個條目,包括漏尿次數、漏尿量、漏尿對日常生活影響程度及漏尿發生的時間[8]。量表總分是前三個條目得分之和,總得分范圍為0~21分,根據總得分劃分UI的嚴重程度,1~5分為輕度,6~12分為中度,13~18分為重度,19~21分為極重度。根據量表第4個條目,可以確定UI的類型:選擇“在咳嗽或打噴嚏時漏尿”“在活動或體育運動時漏尿”任意一項或兩項為壓力性尿失禁(stress urinary incontinence,SUI);選擇“未能到達廁所就會有尿液漏出”“在小便完和穿好衣服時漏尿”任意一項或兩項為急迫性尿失禁(urge urinary incontinence,UUI);同時選擇“在咳嗽或打噴嚏時漏尿”“在活動或體育運動時漏尿”任意一項或兩項以及“未能到達廁所就會有尿液漏出”“在小便完和穿好衣服時漏尿”任意一項或兩項的為混合型尿失禁(mixed urinary incontinence,MUI);選擇“在睡著時漏尿”“在沒有明顯理由的情況下漏尿”“在所有時間內漏尿”的均為其他類型。(3)UI治療意愿調查。有UI癥狀的產婦(ICIQ-SF>0)作答此條目:“您是否愿意接受針對尿失禁癥狀的治療指導”,如選擇“否”則作答下一個條目:“您不愿意接受治療指導的原因是”。有三個選項:目前癥狀不嚴重,沒必要治療;癥狀應該會自行緩解,不需要治療;需要時再來咨詢。固定三名調查員經過統一培訓,在產婦產后6~8周門診產后復查時發放問卷。征得產婦知情同意后,調查員為調查對象解釋調查問卷條目,回收時仔細審核問卷完整性,保證調查的真實性和完整性。
1.3 觀察指標 (1)根據ICIQ-SF簡表調查產婦UI嚴重程度分級及類型分布情況。(2)產褥期UI產婦治療意愿相關影響因素的單因素比較。
1.4 統計學處理 采用SPSS 16.0軟件對所得數據進行統計分析,計量資料用(x±s)表示,比較采用t檢驗;計數資料以率(%)表示,比較采用字2檢驗,P<0.05為差異有統計學意義。
2 結果
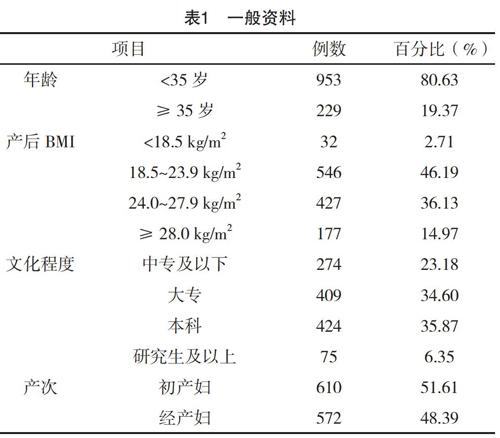
2.1 一般資料 1 250例產婦參加此項調查,回收有效問卷1 182份,問卷有效回收率94.56%。調查產婦年齡16~43歲,平均(30.60±4.10)歲,見表1。
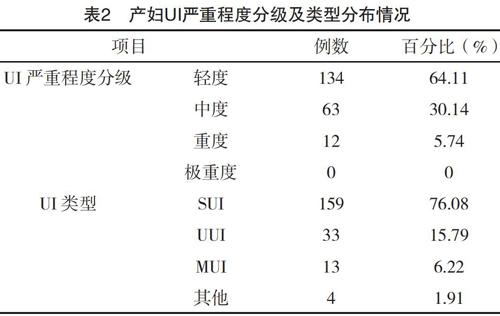
2.2 產褥期產婦UI發生情況 調查的產婦中,17.68%(209/1 182)發生UI,初產婦UI發生率為16.56%(101/610),經產婦UI發生率為18.88%(108/572),絕大多數產婦UI嚴重程度為輕中度,且類型以SUI為主,占76.08%(159/209),見表2。
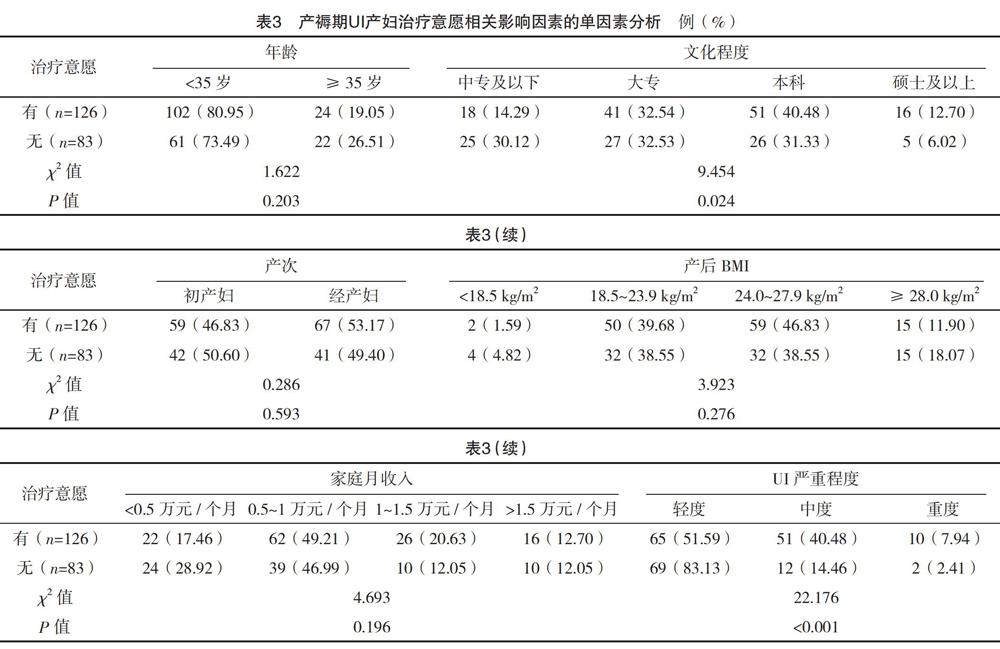
2.3 產褥期UI產婦治療意愿相關影響因素的單因素分析 209例產褥期存在UI的產婦中,126例(60.29%)有治療意愿,83例(39.71%)無治療意愿。無治療意愿產婦中,44.58%(37例)覺得UI癥狀不嚴重,認為沒有治療必要,32.53%(27/83)認為漏尿癥狀應該可以自行恢復,另外有22.89%(19/83)的產婦,想過段時間再考慮。中、重度UI與文化程度高的產婦均更愿意接受UI治療,差異均有統計學意義(P<0.05),見表3。
3 討論
產婦產褥期UI發生率較高,且以SUI為主。本調查結果顯示,產婦產褥期UI的總體發生率為17.68%,其中,經產婦UI發生率略高于初產婦。國際上報道的產婦產后3~6個月UI的發生率在30%左右,遠高于本調查結果[9-11]。考慮本調查醫院剖宮產率較高可能是主要影響因素,有相關研究提示剖宮產是UI的保護因素[7,12-13]。此外,UI篩查工具的不同也是UI發生率低于國外報道的一個方面,是否與調查對象種族、遺傳等因素有關,有待進一步研究。我國的一項多中心流行病學調查結果顯示,初產婦產后6周和產后6個月的UI發生率分別為9.5%和6.8%[14]。另外一項關于北京1 889名初產婦的研究報道,產后6個月UI發生率是9.9%[15]。本研究中UI發生率明顯高于兩項國內研究報道的數據,與兩項研究結果一致的是產婦產后UI均以SUI為主。分析本調查產后UI發生率較高的原因,可能主要與調查人群不同有關,之前的兩項研究調查對象均為年輕的初產婦,隨著社會發展及二胎政策開放,婦女生育年齡延遲,此次調查人群年齡平均(30.60±4.10)歲,高齡產婦占19.37%,且近一半為經產婦。據研究報道,年齡、產次是與UI發生的高危因素[16-18]。另外,本調查發現這部分人群產后6~8周時BMI偏高,36.13%產婦超重,14.97%產婦肥胖,高BMI與UI的發生也有重要關系[19-20]。
另外,在本研究中,產婦產褥期UI以輕中度為主,其中,約64.11%的產婦為輕度UI,30.14%的產婦為中度UI,5.74%為重度,輕中度的UI多可治,一般不需要手術治療。近年來,國內外的研究均表明,分娩和妊娠是UI的重要危險因素,很多UI患者的癥狀都始于孕期或產后[9,17,21]。因此,在產后UI發生率較高的現狀下,臨床有必要在產后復查時盡早開展UI的普及篩查,量表作為簡便易行的篩查工具,可以嘗試在基層醫院推廣。同時針對產后UI中主要類型的SUI的相關高危發病因素進行有效干預,采用適合輕中度UI的保守治療方案,比如國內外推薦的SUI的一線治療方法盆底肌肉訓練(pelvic floor muscle training, PFMT)[22-24],可以作為對產后UI的初級防治措施。
產婦治療意愿不高、UI嚴重程度及產婦文化程度是主要影響因素。盡管UI影響著世界眾多女性的生活質量,但是UI患者主動就醫率卻很低。國內的一項研究結果顯示,接受調查的UI女性中,只有22.1%曾因UI問題咨詢就診[3]。Brown等[5]研究發現在產后一年內,存在尿、糞失禁癥狀的產婦只有不到四分之一的人向醫務人員進行了咨詢。本調查結果顯示,39.71%的產褥期UI產婦不愿意因為UI接受治療指導,本研究未隨訪到產婦后期UI相關的就醫率。家庭及社會支持等因素均會影響到產婦的就醫行為,所以UI產婦的實際就醫率可能會低于治療意愿的數據[25]。本研究發現,UI產婦的治療意愿與UI的嚴重程度密切相關,這與Ros等[26]的研究結果一致。對沒有治療意愿的產婦進一步調查發現,大部分認為漏尿癥狀不嚴重,不需要治療,有的產婦對UI有片面認識,或是對治療持觀望態度,這些現狀都會造成UI產婦錯失最佳的恢復時期。本研究還發現,文化程度高的UI產婦治療意愿強于文化程度低的UI產婦,與對UI的認知程度高有關。所以,臨床工作中需尤其重視對文化程度低、UI程度較輕的產婦的健康教育,多種形式、多途徑的開展宣傳教育工作,提高產婦對UI的認知以及重視程度。
鑒于目前產褥期UI較高的發生率,有必要在基層臨床開展UI的早期篩查,信效度良好的UI量表可以作為一種簡便易行的篩查工具。因產婦UI癥狀總體較輕,產婦治療積極性不高,需針對UI的危害及早期治療重要性加強宣教,圍繞產后UI的臨床特點及產婦需求現狀,進一步探討適宜、可行的UI防治策略。
參考文獻
[1] Susan W,Linda K.Improving Care for Women With Urinary Incontinence in Primary Care[J].The Journal for Nurse Practitioners,2017,13(10):675-680.
[2]李琳,朱蘭,郎景和,等.中國成年女性混合性尿失禁的流行病學調查[J].中華醫學雜志,2010,90(21):1487-1490.
[3] Xu D,Wang X,Li J,et al.The mediating effect of bothersome urinary incontinence on help-seeking intentions among community-dwelling women[J].J Adv Nurs,2015,71(2):315-325.
[4] Vethanayagam N,Orrell A,Dahlberg L,et al.Understanding help-seeking in older people with urinary incontinence: An interview study[J].Health Soc Care Community,2017,25(3):1061-1069.
[5] Brown S,Gartland D,Perlen S,et al.Consultation about urinary and faecal incontinence in the year after childbirth:a cohort study[J].BJOG,2015,122(7):954-962.
[6] Viktrup L.The risk of lower urinary tract symptoms five years after the first delivery[J].Neurourol Urodyn,2002,21(1):2-29.
[7] MacArthur C,Wilson D,Herbison P,et al.Urinary incontinence persisting after childbirth: extent, delivery history, and effects in a 12-year longitudinal cohort study[J].BJOG,2016,123(6):1022-1029.
[8] Avery K,Donovan J,Peters T J,et al.ICIQ:a brief and robust measure for evaluating the symptoms and impact of urinary incontinence[J].Neurouol Urodyn,2004,23(4):322-330.
[9] Thom D H,Rortveit G.Prevalence of postpartum urinary incontinence:a systematic review[J].Act Obstet Gynecol Scand,2010,89(12):1511-1522.
[10] Rocha J,Brand?o P,Melo A,et al.Assessment of Urinary Incontinence in Pregnancy and Postpartum:Observational Study[J].Acta Med Port,2017,30(7-8):568-572.
[11] Ayten D,Sibel O,Merve?elik M D.Examining prevalence of urinary incontinence and risk factors in women in third postpartum month[J].International Journal of Urological Nursing,2019,13(1):13-22.
[12] Blomquist J L,Mu?oz A,Carroll M,et al.Association of Delivery Mode With Pelvic Floor Disorders After Childbirth[J].JAMA,2018,320(23):2438-2447.
[13] T?htinen R M,Cartwright R,Tsui J F,et al.Long-term Impact of Mode of Delivery on Stress Urinary Incontinence and Urgency Urinary Incontinence: A Systematic Review and Meta-analysis[J].Eur Urol,2016,70(1):148-158.
[14] Zhu L,Li L,Lang J H,et al.Prevalence and risk factors for peri-and postpartum urinary incontinence in primiparous women in China:a prospective longitudinal study[J].Int Urogynecol J,2012,23(5):563-572.
[15] Yang X,Zhang H X,Yu H Y,et al.The prevalence of fecal incontinence and urinary incontinence in primiparous postpartum Chinese women[J].Eur J Obstet Gynecol Reprod Biol,2010,152(2):214-217.
[16] Zhou H H,Shu B,Liu T Z,et al.Association between parity and the risk for urinary incontinence in women:A meta-analysis of case-control and cohort studies[J].Medicine(Baltimore),2018,97(28):e11443.
[17]嚴文廣,李旭紅,孫紹丹,等.女性盆腔臟器脫垂和尿失禁的危險因素[J].中南大學學報(醫學版),2018,43(12):1345-1350.
[18]余昆,余志海,劉勝,等.中國成年女性尿失禁患病率的meta分析[J].中國循證醫學雜志,2019,19(1):36-43.
[19] Vissers D,Neels H,Vermandel A,et al.The effect of non-surgical weight loss interventions on urinary incontinence in overweight women: a systematic review and meta-analysis[J].Obesity Reviews,2014,15(7):610-617.
[20] Lee U J,Kerkhof M H,van Leijsen S A,et al.Obesity and pelvic organ prolapse[J].Curr Opin Urol,2017,27(5):428-434.
[21] Schreiber Pedersen L,Lose G,H?ybye M T,et al.Prevalence of urinary incontinence among women and analysis of potential risk factors in Germany and Denmark[J].Acta Obstet Gynecol Scand,2017,96(8):939-948.
[22] Qaseem A,Dallas P,Forciea M A,et al.Nonsurgical management of urinary incontinence in women:a clinical practice guideline from the American College of Physicians[J].Ann Intern Med,2014,161(6):429-440.
[23] Dumoulin C,Hay-Smith J,Habée-Séguin G M,et al.Pelvic floor muscle training versus no treatment,or inactive control treatments,for urinary incontinence in women:a short version Cochrane systematic review with meta-analysis[J].Neurourol Urodyn,2015,34(4):300-308.
[24]孫智晶,朱蘭,郎景和,等.盆底肌肉訓練在盆底功能障礙性疾病防治中的作用[J].中華婦產科雜志,2017,52(2):138-140.
[25] Fritel X,Panjo H,Varnoux N,et al.The individual determinants of care-seeking among middle-aged women reporting urinary incontinence:analysis of a 2273-woman cohort[J].Neurourol Urodyn,2014,33(7):1116-1122.
[26] Ros C,Espu?a-Pons M,Ortega J A,et al.Urinary incontinence in gynaecological consultations.Do all women with symptoms wish to be treated?[J].Actas Urol Esp,2015,39(10):628-634.
(收稿日期:2019-03-07) (本文編輯:田婧)
