骨質疏松癥患者危險因素分析及雙能X射線骨密度儀檢測掃描身體脂肪量增加與骨質丟失相關性分析
2017-12-02 01:59:11羅一博權建平
中國醫學裝備 2017年11期
關鍵詞:分析
蓋 福 羅一博 權建平 閆 軍
骨質疏松癥患者危險因素分析及雙能X射線骨密度儀檢測掃描身體脂肪量增加與骨質丟失相關性分析
蓋 福①羅一博①權建平①閆 軍②*
目的:探討骨質疏松癥患者危險因素,并應用雙能X射線骨密度儀檢測掃描骨質疏松癥患者身體脂肪量增加與骨質丟失相關性。方法:選取醫院收治的700例骨質疏松癥患者,給予所有患者至少2次雙能X射線檢測儀檢測體脂含量和骨密度情況,分析骨質疏松癥患者骨折史及骨折危險因素,不同身體質量指數(BMI)患者身體脂肪量變化與骨密度指數T值變化情況,以及骨質疏松癥患者脂肪量與骨密度T值相關性。結果:線性回歸分析結果顯示骨密度指數T值變化、骨盆骨折史、股骨骨折史以及炎癥疾病史是骨質疏松癥患者的危險因素;不同BMI組患者體脂含量變化數據比較,其差異無統計學意義(F=0.786,P>0.05),不同BMI患者骨密度指數T值變化數據比較,其差異無統計學意義(F=0.963,P>0.05);Logistics回歸分析結果顯示,骨質疏松癥患者脂肪量增加與骨密度指數T值呈顯著正相關(r=0.563,P<0.05)。結論:雙能X射線骨密度儀檢測掃描分析能夠準確反映骨質疏松癥患者的體脂含量,骨質疏松癥患者適當增加體脂含量,有利于增加骨密度,減少骨折風險。
雙能X射線;骨密度;骨質疏松癥;脂肪量;骨質丟失
骨質疏松癥被認為是系統性的骨骼疾病,主要表現為低骨量以及基礎骨組織不斷惡化,導致骨質脆弱,易骨折[1-2]。近年來,骨質疏松癥的發病率和病死率呈逐年上升趨勢,全球現有患者已接近600萬,被世界衛生組織公認為嚴重威脅人類健康的疾病之一[3]。骨質疏松癥的治療以預防為主,通過一系列工具評估可能的風險,以便進行有效的針對性預防治療[4]。為此,本研究對700例骨質疏松癥患者應用雙能X射線骨密度儀檢測掃描進行觀察分析,探討骨質疏松癥患者身體脂肪量增加與骨質丟失相關性。
1 資料與方法
1.1 一般資料
回顧性分析2010年1月至2014年1月寶雞市人民醫院收治的700例骨折疏松癥患者,其中男性98例,女性602例;年齡20~86歲,平均年齡(64.5±11.3)歲;所有患者均進行至少兩次的雙能X射線檢測儀檢測體脂含量和骨密度情況,檢測間隔時間0.1~5.0年,平均間隔(3.0±0.9)年。第一次檢測骨密度指數T值為-1.8~5.0,平均T值(1.1±1.2),第二次檢測骨密度指數T值為-2.4~4.6,平均T值(1.4±0.5);脂肪量變化-17.8%~22.8%,平均變化(-2.9±18.8)%,本研究經醫院倫理委員會討論后通過,所有患者及其家屬知情后簽署知情同意書。
1.2 納入與排除標準
(1)納入標準:①明確的骨質疏松癥診斷;②年齡18~90歲。
(2)排除標準:①合并有影響骨密度的疾病;②長期服用影響骨密度的藥物;③未能隨訪或資料缺失。
1.3 檢測方法
(1)收集700例患者的病史情況,包括患者的習慣性用藥史、家族史、胃腸疾病、炎癥疾病、惡性腫瘤、謝性疾病、類風濕性關節炎、吸煙史及皮質類固醇使用等情況,對習慣性用藥的患者重點關注可能影響骨密度的藥物,統計所有骨質疏松癥患者的骨折史。
(2)體脂和骨密度掃描:采用雙能X射線骨密度檢查儀(美國Hologic公司)掃描,患者平臥于檢查床,從頭側向足側掃描,范圍寬度固定為60 cm,并根據患者的身高設定掃描長度,時間約為5 min,記錄患者的身高、體重、總體脂含量以及骨密度情況。骨密度指數采用T值法,計算為公式1:

脂肪含量變化計算為公式2:

1.4 評價指標
分別統計女性和男性骨質疏松癥患者危險因素及骨折史,分析骨質疏松癥患者危險因素,不同身體質量指數(body mass index,BMI)患者身體脂肪量變化與骨密度指數T值變化情況以及脂肪量變化與骨密度指數T值相關性。
1.5 統計學方法
采用SPSS18.0軟件對數據進行統計分析,計量資料以均值±標準差(±s)表示,多組間計量資料比較采用F檢驗,骨質疏松癥患者危險因素采用線性回歸分析,骨質疏松癥患者脂肪量變化與骨密度指數T值相關性分析采用logistics回歸分析,以P<0.05表示差異有統計學意義。
2 結果
2.1 骨質疏松癥患者危險因素及骨折史分析
統計700例骨質疏松癥患者的危險因素,主要包括習慣性用藥史、家族史、胃腸疾病、炎癥疾病、惡性腫瘤、謝性疾病、類風濕性關節炎、吸煙史及皮質類固醇使用等;骨折部位主要為股骨、前臂、肱骨、骨盆、肋骨、脊柱以及脛骨和(或)腓骨等,見表1。

表1 骨質疏松癥患者危險因素及骨折史分析[例(%)]
2.2 骨質疏松癥患者危險因素線性回歸分析
線性回歸分析結果顯示,骨密度指數T值變化、骨盆骨折史、股骨骨折史以及炎癥疾病史是骨質疏松癥患者的危險因素,見表2。
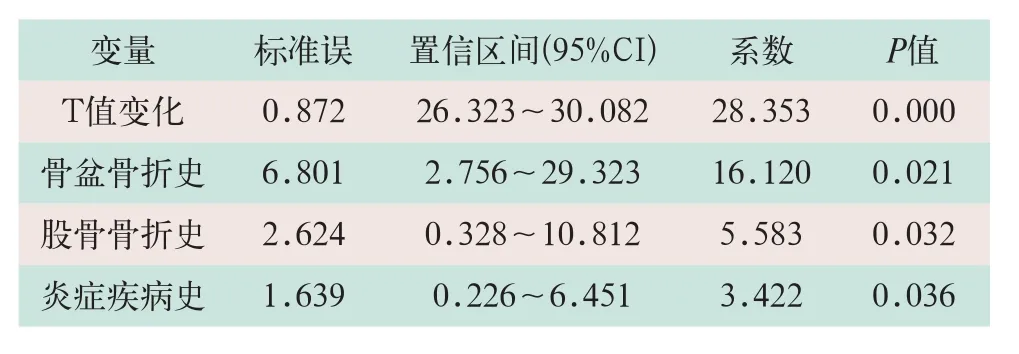
表2 骨質疏松癥患者危險因素分析
2.3 不同BMI患者身體脂肪量變化與骨密度指數T值變化情況分析
不同BMI患者體脂含量變化數據比較,其差異無統計學意義(F=0.786,P>0.05);不同BMI患者骨密度指數T值變化數據比較,其差異無統計學意義(F=0.963,P>0.05),如圖1所示。
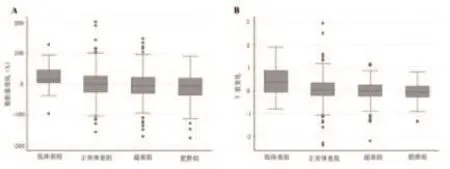
圖1 不同BMI患者身體脂肪量變化與骨密度指數T值變化情況分析示圖
2.4 骨質疏松癥患者脂肪量變化與骨密度指數T值相關性回歸分析
Logistics回歸分析結果顯示,骨質疏松癥患者脂肪量增加與骨密度指數T值呈顯著正相關(r=0.563,P<0.05),如圖2所示。
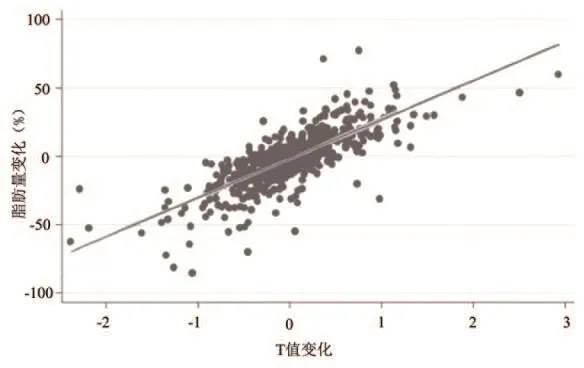
圖2 骨質疏松癥患者脂肪量變化與骨密度指數T值相關性回歸分析示圖
3 討論
長期以來,國際上通常采用BMI反映人體的肥胖程度,雖然該方法具有簡單、實用、經濟等優點,但是缺點也比較明顯,不能反映身體的局部脂肪分布和脂肪含量。因此,尋找一種更準確、更科學的反映身體脂肪含量的方法更為重要。雙能X射線骨密度儀采用筆束式快速掃描的方式,能夠進行快速準確定位,且測量精度較高。不僅能準確反映骨密度情況,還能夠對人體的上肢、下肢和軀干部位的脂肪異常分布能進行客觀的評價,進而對人體內的總體脂肪含量進行評估,同時還能獲得體內非脂肪含量和分布的信息,臨床應用價值高[5]。
本研究結果顯示,既往骨折史是骨質疏松發生的危險因素。其可能原因是骨折史導致患者骨骼肌肉系統創傷引起骨折部位及周邊局部的骨量喪失,導致骨質疏松,有可能進一步引起骨質疏松性骨折,造成骨量丟失,形成惡性循環。此外,骨折后長期臥床及制動也可能引起骨量丟失。相關研究表明,骨折后6個月,患者的骨量呈持續減少趨勢,且恢復期較長。而椎體、髖部等部位發生骨折后,再次發生骨折的概率顯著增加[6-7]。
本研究結果顯示,骨質疏松癥患者脂肪量增加均與骨密度指數T值呈顯著正相關,且不受BMI范圍的影響。以往研究認為BMI是獨立骨質疏松癥的危險因素,較低BMI顯著增加骨質疏松癥發生風險,體重和身體成分變化也是骨折風險的不良因素[8]。但這一觀點尚存在爭議,如在女性患者中的低BMI患者,發生髖部骨折的風險較高,研究認為,與脂肪組織分泌的一些調節因子有關,而有研究表明,BMI對骨質疏松癥的影響僅適應于低BMI患者,對于其他類別的患者則呈相反的結論[9-10]。此外,相關研究結果顯示,肌肉組織的含量并不與BMI正相關,推測肌肉組織的含量是骨質疏松癥的保護性因素,但尚未得到確認[11]。因此,BMI并不是一個準確反映身體形態的有效測量工具,也不能準確分析身體成分的變化及其對骨密度的影響[12]。通過干預骨質疏松癥患者的生活方式來適度增加體脂含量,有利于降低骨折風險。然而,不容忽視的是增加體脂肪量與心血管疾病的發生風險是顯著相關的,為了避免增加心血管疾病的風險,醫生可以審慎的建議BMI<18.5和年齡>60歲的患者適量增加體脂肪量。研究認為,脂肪組織可分泌一系列調節因子參與骨質調控,其中包括瘦素、雌激素及脂聯素等因子,能夠降低破骨細胞的活性,加強小腸對鈣的吸收能力,并降低骨骼中的鈣流失,維持骨量和骨質量[13-14]。此外,體脂含量的增加能夠增加骨骼的機械應力,進而增加骨密度[15]。
有報道認為,長期吸煙可明顯降低骨密度,進一步發生骨質疏松。但本研究中絕大多數為女性患者,且吸煙比例較低,因此,本研究并未深入探討吸煙對骨質疏松癥的影響[16]。
雙能X射線骨密度儀檢測掃描分析能夠準確反映骨質疏松癥患者的體質含量,骨質疏松癥患者應適當增加體脂含量,有利于增加骨密度,減少骨折風險。
[1]李國新.老年胸腰椎移行部骨折并骨質疏松癥的非手術綜合治療[J].河北醫藥,2015,37(14):2138-2140.
[2]Salemyr M,Muren O,Ahl T,et al.Lower periprosthetic bone loss and good fixation of an ultrashort stem compared to a conventional stem in uncemented total hip arthroplasty[J].Acta Orthopaedica Scandinavica,2015,108(6):1877-1888.
[3]Stein EM,Kepley A,Walker M,et al.Skeletal Structure in Postmenopausal Women With Osteopenia and Fractures Is Characterized by Abnormal Trabecular Plates and Cortical Thinning[J].J Bone Miner Res,2014,29(5):1101-1109.
[4]汪清華,賴俊成,胡益雄,等.老年性骨質疏松癥患者骨折的相關因素分析[J].牡丹江醫學院學報,2016,37(4):54-56.
[5]王立童,辛玉英,張淑榮,等.雙能X線吸收測量法(DEXA)測定成年人單純性肥胖癥脂肪含量研究[J].中山大學學報(自然科學版),2009,48(2):95-98.
[6]Villalon KL,Gozansky WS,Van Pelt RE,et al.A Losing Battle:Weight Regain Does Not Restore Weight Loss-Induced Bone Loss in Postmenopausal Women[J].Obesity (Silver Spring),2011,19(12):2345-2350.
[7]Lee HR,Hong SS,Lee SY,et al.The Impact of Body Weight Change on Bone Mineral Density of the Lumbar Spine in Perimenopausal Women:A Retrospective,One-year Follow-up Study[J].Korean J Fam Med,2011,32(4):219-225.
[8]Cummins NM,Poku EK,Towler MR,et al.clinical risk factors for osteoporosis in Ireland and the UK:a comparison of FRAX and QFractureScores[J].Calcif Tissue Int,2011,89(2):172-177.
[9]Trémollieres FA,Pouillès JM,Drewniak N,et al.Fracture risk prediction using BMD and clinical risk factors in early postmenopausal women:sensitivity of the WHO FRAX tool[J].J Bone Miner Res,2010,25(5):1002-1009.
[10]王慧.類風濕關節炎患者骨質疏松性骨折風險FRAX評估的研究進展[J].安徽醫學,2014,35(1):137-139.
[11]Dam TT,Peters KW,Fragala M,et al.An evidencebased comparison of operational criteria for the presence of sarcopenia[J].J Gerontol,2014,69(5):584-590.
[12]Sirola J,Rikkonen T,Tuppurainen M,et al.Should risk of bone fragility restrict weight control for other health reasons in postmenopausal women?--A ten year prospective study[J].Maturitas,2011,71(2):162-168.
[13]van den Bergh JP,van Geel TA,Lems WF,et al.Assessment of individual fracture risk:FRAX and beyond[J].Curr Osteoporosis Rep,2010,8(3):131-137.
[14]Bratland-Sanda S,Martinsen EW,Sundgot-Borgen J.Changes in physical fitness,bone mineral density and body composition during inpatient treatment of underweight and normal weight females with longstanding eating disorders[J].Int J Environ Res Public Health,2012,9(1):315-330.
[15]Hedges WP,Bukhari M.Increasing body fat mass reverses bone loss in osteopenia as detected by dual-energy X-ray absorptiometry scans[J].Eur J Rheumatol,2016,3(1)1-4.
[16]Oldroyd A Mitchell K,Bukhari M.The prevalence of osteoporosis in an older population with very high body mass index:evidence for an association[J].Int J Clin Pract,2014,68(6):771-774.
A analysis of risk factors for osteoporosis and a correlation analysis between increasing of body fat and losing of sclerotin by using bone mineral densimeter of Dual energy X-ray
GAI Fu, LUO Yi-bo, QUAN Jian-ping, et al
Objective:To investigate the risk factors of patients with osteoporosis, and to apply bone mineral densimeter of Dual energy X-ray to scan increasing of body fat and losing of sclerotin of these patients and analyze their correlation.Methods:700 patients with osteoporosis
scans by using bone mineral densimeter of Dual energy X-ray at least 2 times to detect the content of body fat and situation of bone mineral density. The fracture history and risk factors of fracture of patients with osteoporosis were analyzed, and the change of body fat and change of T index of patients with different BMI were analyzed. Besides, the correlation between body fat and T value of patients with osteoporosis also was analyzed and researched.Results:The linear regression analysis indicated that the risk factors of patients with osteoporosis included the change of T value, fracture history of pelvis,fracture history of femur and diseases history of inflammation. The differences of the changes of body fat among different BMI groups were no significant (F=0.786, P>0.05), and the differences of T value among different BMI groups also were no significant (F=0.963, P>0.05). The results of Logistics regression analysis indicated that there was a significant positive correlation between the increasing of body fat and T value in patients with osteoporosis(r=0.563, P<0.05).Conclusion:The bone mineral densimeter of Dual-energy X-ray can accurately reflect the content of body fat of osteoporosis patients. And the appropriate increasing of body fat of them is benefit for the increasing of bone mineral density and reducing of the risk of fracture.
Dual energy X-ray; Bone mineral density; Osteoporosis; Fat mass; Bone loss
Department of Radiotherapy, Baoji People's Hospital, Baoji 721000, China.
1672-8270(2017)11-0061-04
R812.4
A
10.3969/J.ISSN.1672-8270.2017.11.018

蓋福,男,(1982- ),本科學歷,主治醫師。寶雞市人民醫院放射科,研究方向:數字化胃鏡造影。
①寶雞市人民醫院放射科 陜西 寶雞 721000
②延安大學附屬醫院放射科 陜西 延安 716000
*通訊作者:fyyanjun@163.com
China Medical Equipment,2017,14(11):61-64.
2017-06-04
猜你喜歡
現代畜牧科技(2021年9期)2021-10-13 06:39:14
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
電子制作(2018年18期)2018-11-14 01:48:24
山東工業技術(2016年15期)2016-12-01 05:31:22
當代經濟研究(2016年5期)2016-12-01 03:12:05
現代農業(2016年5期)2016-02-28 18:42:46
出版與印刷(2016年3期)2016-02-02 01:20:11
中國中醫藥現代遠程教育(2014年11期)2014-08-08 13:23:44
華北水利水電大學學報(社會科學版)(2014年3期)2014-04-16 04:38:31
終身教育研究(2014年5期)2014-02-28 01:23:06
