Efficacy comparison between anterior subcutaneous and submuscular transposition of ulnar nerve in treating moderate-severe cubital tunnel syndrome
2017-11-08 01:22:19HungWei黃偉ChenQunxin陳全新WuMeiho吳美超QuTinge曲天歌WngFeifei王菲菲Jie馬杰CiLingling蔡玲玲
Hung Wei(黃偉), Chen Qunxin(陳全新),Wu Meiho(吳美超), Qu Tin’ge(曲天歌),Wng Feifei(王菲菲), M Jie(馬杰), n Ci Lingling(蔡玲玲)*
a: Shanxian County Center Hospital of Shandong Province,Heze 274300, China
b: Dongfang Hospital, the Second Affiliated Hospital of Beijing University of Chinese Medicine, Beijing 100078, China
c: Dongzhimen Hospital, the First Affiliated Hospital of Beijing University of Chinese Medicine, Beijing 100700, China
d: School of Graduates, Beijing University of Chinese Medicine,Beijing 100029, China
Efficacy comparison between anterior subcutaneous and submuscular transposition of ulnar nerve in treating moderate-severe cubital tunnel syndrome
Huang Wei(黃偉)a, Chen Quanxin(陳全新)a,Wu Meichao(吳美超)b, Qu Tian’ge(曲天歌)c,Wang Feifei(王菲菲)d, Ma Jie(馬杰)d, and Cai Lingling(蔡玲玲)b*
a: Shanxian County Center Hospital of Shandong Province,Heze 274300, China
b: Dongfang Hospital, the Second Affiliated Hospital of Beijing University of Chinese Medicine, Beijing 100078, China
c: Dongzhimen Hospital, the First Affiliated Hospital of Beijing University of Chinese Medicine, Beijing 100700, China
d: School of Graduates, Beijing University of Chinese Medicine,Beijing 100029, China
OBJECTIVE:To explore the optimal surgery in treating moderate-severe cubital tunnel (CuTS) syndrome by comparing the clinical efficiency of decompression and anterior subcutaneous transposition of ulnar nerve and decompression and anterior submuscular transposition of ulnar nerve, and to provide a theoretical basis for the appropriate surgical programs in treating moderate-severe CuTS.
METHODS:47 consecutive cases of moderate-severe CuTS were surgically treated in our department from January 2014 to January 2017.All patients were divided into two groups by the doctor in our department. 21 CuTS cases were treated with decompression and anterior subcutaneous transposition of ulnar nerve, and other 26 cases were treated with decompression and anterior submuscular transposition of ulnar nerve. All the patients were followed 1 month, 3 months and 6 months after operation to evaluate the recovery degree of ulnar nerve function and the clinical efficiency of the two methods was compared.
RESULTS:Clinical symptoms of two groups were significant alleviated. There was no significant statistical difference between two groups in the clinical efficiency.
CONCLUSION:Completely releasing of nerve truck is the most important step in treating mediate-severe CuTS. The clinical results of the two methods are similar, but the anterior subcutaneous transposition of ulnar nerve is more easy to operate and can be widely used.
Cubital tunnel syndrome; Anterior subcutaneous transposition of ulnar nerve;Anterior submuscular transposition of ulnar nerve
The cubital tunnel syndrome (CuTS) is the second most frequent peripheral nerve entrapment syndrome after carpal tunnel syndrome. If the clinical features of CuTS are results of pressure from surrounding anatomic structure, the clinical effect of conservative treatment would be poor. Surgery is recommended in case where conservative measurements have failed. The most commonly described methods of surgery which are reported in literatures are: (1)Ulnar nerve release, (2)decompression and anterior subcutaneous transposition of ulnar nerve, (3)decompression and anterior submuscular transposition of ulnar nerve. Method of ulnar nerve release has almost been eliminated, and the latter two are now wildly used. The purpose of this randomized study is to evaluate the clinical outcome of subcutaneous and submuscular transposition of ulnar nerve. Here is the report.
PATIENTS AND METHODS
Research subjects
Forty-seven patients with mediate-severe CuTS were included in our study from January 2014 to January 2017 in our department. All patients were randomly divided into two groups, group A and group B. 21 CuTS cases were treated with decompression and anterior subcutaneous transposition of ulnar nerve (group A),and the other 26 cases were treated with decompression and anterior submuscular transposition of ulnar nerve(group B). In group A, there were 17 males and 4 females, aged 28-65 years (mean 48.5 years). In group B, there were 21 males and 5 females, aged 40-62 years (mean 51 years). Among all participants, 3 cases had previous history of elbow trauma, the rest were not obviously incentive. Patients had disease history of three months to 10 years. The follow-up time was 1 month, 3 months and 6 months after operation.
Symptoms
The ulnar nerve dysfunction of all patents has been evaluated by Dellon classification: mild: paraesthesia is intermittent; normal two point discrimination;subjective weakness, clumsiness, or loss of coordination tests;elbow flexion test, Tinel sign, or both are positive.Moderate: paraesthesia is intermittent,vibratory perception normal or decreased;measurable weakness in pinch or grip strength tests;elbow flexion test,Tinel sign, or both are positive; finger crossing may be abnormal. And severe: Paraesthesia is persistent;vibratory perception decreased; abnormal two point discrimination; measurable weakness in pinch or grip strength plus muscle atrophytests; elbow flexion test, Tinel sign, or both are positive; finger crossing usually abnormal. All patients were classified as suffering from moderate or severe CuTS. There were no significant differences in age, sex, pathogenicity and severity of disease between the two groups.
Surgical techniques
Anesthesia and position: All patients were performed brachial plexus block and putted in supine position with the arm abducted at 70°. A brachial tourniquet, inf l ated to 260 mmHg, was used for all surgeries.
Steps: Involved upper extremities was disinfected with iodophor and sterile drapes, then covered with a mask. A skin incision, of which the proximal was near to 7cm and distal was near to 5cm, was centered at the medial epicondyle. The ulnar nerve was looked for in the medial candyle behind the ulnar nerve groove after separating from cutaneous, subcutaneous to deep fascia in turn, and protected by pulling with a rubber strip. The nerve was released at the medial intermuscular septum from nerbiduct. In the process of ulnar nerve exposure,the blood vessels that associated with the nerve should be well protected,the small ulnar branches of the ulnar nerve should to be severed and motor nerve fibers of fl exor carpi ulnaris were forbidden to damage. If scar or fibrous hyperplasia was found, decompression should be performed by cutting the epineurium.
After the nerve truck was fully released, group A was performed anterior subcutaneous transposition, which included shifting the ulnar nerve trunk to the fascia surface in front of entepicondyle of humerus and lifting the fascia layer on the surface of fl exor tendons. Then the ulnar nerve and subcutaneous tissue was fixed by figure-of-eight suture and made sure without new stuck occurred. Group B was performed anterior submuscular transposition, in which the initial parts of pronator teres and fl exor were sharp cut offafter the ulnar nerve was abundant released, and then the muscle groups was turned to the anterolateral of elbow without injuring the nervi medianus.2 holes were drilled at the medial condyle, and the muscles were fixed to the medial condyle with 2-0 tendon sutures after shifting the ulnar nerve in the muscles.These methods of surgery should ensure the nerve inlet was without compression during operation.The diameter for the nerve inlet was advisable to fit a little finger.
Two groups of patients were to maintain the elbow flexion 90° and splint fixed after operation which was removed offsplint 10 day later. Patients could perform active exercise under the protection of the sling, but should avoid edpronation and supination activities of forearm.
CLINICAL OUTCOMES
Patient functional status like sensory and motor was divided into four grades by using Yudong Gu function assessment 1 month, 3 months, 6 months after surgery.
STATISTICAL ANALYSIS
The results were analyzed using SPSS19.0.Measurement data were indicated as “mean value± standard deviation”(x±s). We used t-test to analyze measurements which conformed with normal distributions and non-parametric test to analyze measurements which conformed with non-normal distributions. We used chi-square test to analyze enumeration data.There were statistical differences(P<0.05), and there were significant statistical differences (P<0.01).
RESULT
The was no significant difference in excellent and good rate(P>0.05), also in sensory, Tinel sign and the test of finger crossing.
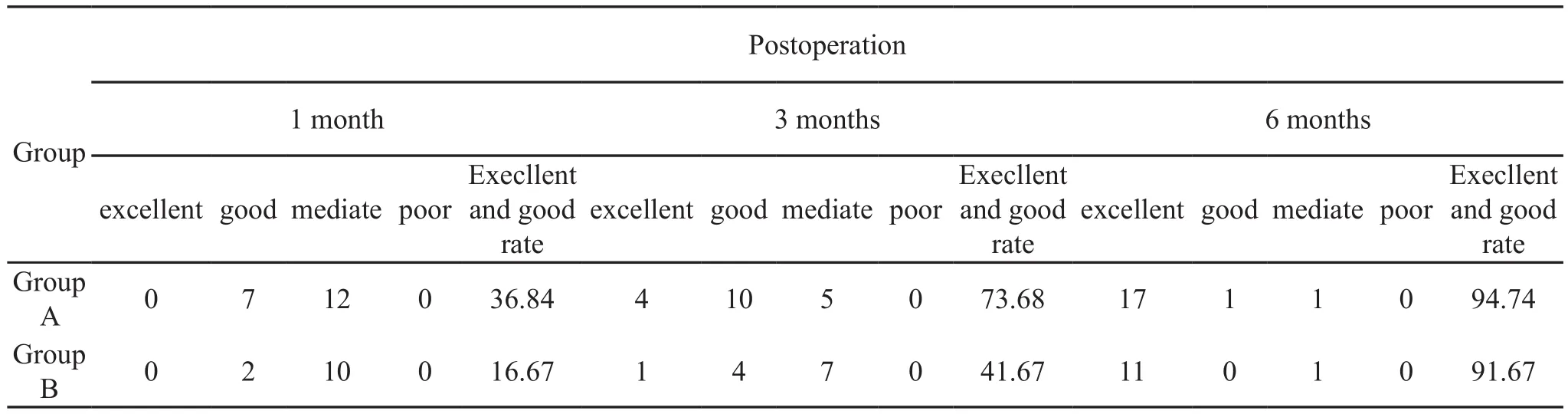
Postoperation 1 month 3 months 6 months Group Execllent and good rate Group A 0 7 12 0 36.84 4 10 5 0 73.68 17 1 1 0 94.74 Group B 0 2 10 0 16.67 1 4 7 0 41.67 11 0 1 0 91.67 excellent good mediate poor Execllent and good rate excellent good mediate poor Execllent and good rate excellent good mediate poor
23 cases of all postoperative patient were follow-up on 1 month, 3 months, 6 months. According to Yudong Gu function assessment, the excellent and good rate of the clinical outcome of the two groups was 94.47%and 91.67%, which there was meant no significant difference on the long-term recovery. But the excellent and good rates of group A and group B on 1 month were 36.84%、and 16.67%, and on 3 months were 73.68%and 41.67% respectively, according to Yudong Gu function assessment, which represented group B was superior to group A on the short-term recovery (table 1).
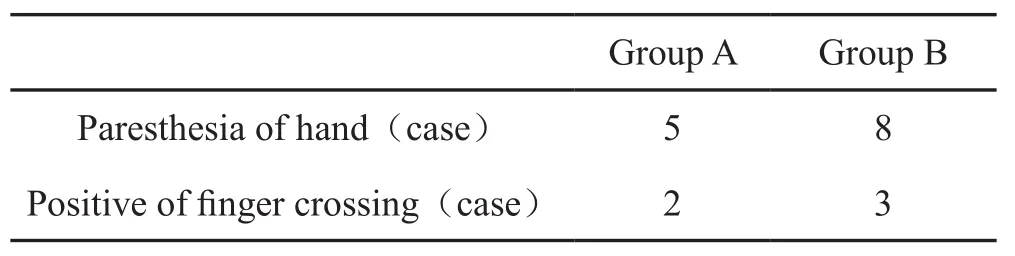
Group A Group B Paresthesia of hand(case) 5 8 Positive of finger crossing(case) 2 3
DISCUSSION
Clinically, mediate-severe CuTS patients always have long-lasting impairment, and would affect the function of dominant muscle due to nerve damage. The recovery of damaged muscles is slow which makes the treatment much difficult. Therefore, the diagnosis and treatment should be performed at early stage.For example, patient should have a surgery once the intrinsic muscle of hand was impaired which represents mediate to severe grade. Three groups of techniques are used most frequently, namely simple decompression,anterior transposition(subcutaneous, intramuscular and submuscular)and medial epicondilectomy.Previous researches have confirmed the clinical efficacy of anterior submuscular transposition of ulnar nerve. Longterm follow-up showed low recurrence rate, and a few patients were with elbow joint contracture. In this study,we evaluate the clinical efficiency of decompression and anterior subcutaneous transposition of ulnar nerve and decompression and anterior submuscular transposition of ulnar nerve by statistical analysis, which might provide surgical treatment evidence for CuTS.
In our research, the ulnar nerve, which stuck in the elbow, was completely decompressed and no significant difference was found in the symptom recovery.Clinically, the best surgical technique for CuTS depended on many factors, for example, the surgical practice of surgeons, the etiology, or the anatomy of the elbow. In our opinion, we prefer anterior subcutaneous transposition for obese patients; otherwise, we are more inclined to the anterior submuscular transposition.
In conclusion, there was no significant difference in hand sensory and motor recovery in the treatment of cubital tunnel syndrome through decompression and anterior subcutaneous transposition of ulnar nerve or decompression and anterior submuscular transposition of ulnar nerve. Which kind of operation should we choose depends on the skill and surgical practice of surgeons and the anatomical features of patient. Two groups,which had surgical treatment in our study,had achieved good clinical results. Clinically, we should choose the most appropriate surgical methods according to specific situation of the patient.
1 Gu YD, Chen DS, Shi QL, et al. Clinical analysis of 128 patients with carpal tunnel syndrome. Chin J Hand Surgery,2006, 22(5):283-285.
2 Gu YD. Current status and suggestion of clinical classification of carpal and cubital tunnel syndromes. Chin J Orthopaedics, 2011, 31(7):818-819.
3 Song XY, Gu YD, He CQ,et al. Application of carpal tunnel release in metacarpus. Chin J Clinical Anatomy, 1999,17(1):50-51.
4 SLATER R R R, BYNUM D K D. Diagnosis and treatment of carpal tunnel syndrome. Orthop Rev, 1993, 22(10): 1095-1105.
5 Acute carpal tunnel syndrome. Hand Clin, 1998, 14(3):419-429.
6 Gu YD. Diagnosis of carpal tunnel syndrome. Orthopedic J China, 2005, 13(5):2-3.
7 Nanavati N, Walker-Bone K, Stanworth H, et al. Outcomes of opencarpal tunnel decompression. N Z Med J, 2013,126(1369):60-67.
*Corresponding author:Email: Lingling89159166@126.com;Mobile phone: +86-13488716861
(Accepted: March 15, 2017)
登錄APP查看全文
 World Journal of Integrated Traditional and Western Medicine
2017年2期
World Journal of Integrated Traditional and Western Medicine
2017年2期
- World Journal of Integrated Traditional and Western Medicine的其它文章
- Clinical study of prevention of urine retention after subabdominal surgery by electro-acupuncture acupoints Yin Ling Quan(SP 9), Zhao Hai(KI 6) with the assistance of subarachnoid acupoint anesthesia
- Clinical study of Cangbai Shiduqing Granul in reversing drug resistance of ureaplasma urealyticum
- INSTRUCTION FOR AUTHORS
- Research progress of Chinese medicine in treatment of IPF(idiopathic pulmonary fibrosis)
- Study and Discussion on Acupuncture Treatment of Urticaria