龜頭包皮炎患者淋病奈瑟菌分離與鑒定及其耐藥機制研究
2017-06-09 09:44:06葛玉梅胡慶豐朱永澤周永列呂火烊
中國人獸共患病學報 2017年5期
葛玉梅,胡慶豐,朱永澤,周永列,呂火烊
?
龜頭包皮炎患者淋病奈瑟菌分離與鑒定及其耐藥機制研究
葛玉梅,胡慶豐,朱永澤,周永列,呂火烊
目的 分離鑒定龜頭化膿性包皮炎病原菌,檢測分離菌株耐藥性并了解其耐藥機制。方法 采取尿道分泌物及龜頭膿包液標本,革蘭染色鏡檢并采用Mycoplasma IST 2試劑盒檢測支原體。上述標本接種哥倫比亞血平板、淋病奈瑟菌選擇平板、酵母菌鑒定平板進行細菌分離培養,獲得的菌落用VITEK 2-compact全自動細菌檢測分析系統進行鑒定,另采用PCR檢測上述標本及菌落的淋病奈瑟菌16S rRNA基因。采用K-B法檢測分離菌株對5種常用抗生素的敏感性,采用β-內酰胺酶和超廣譜β-內酰胺酶確證試驗了解該菌株產酶情況,PCR檢測該菌株耐藥相關tetM、TEM、mefA和ermF基因。 結果 各標本支原體檢測結果均為陰性。尿道分泌物標本分離培養結果均為陰性,龜頭膿包液血平板和選擇平板培養結果為陽性。VITEK 2-compact系統和16S rRNA-PCR檢測結果顯示分離菌株為淋病奈瑟菌。該菌株產β內酰胺酶且對青霉素G、環丙沙星、四環素耐藥,其基因組攜帶tetM、TEM、mefA和ermF基因。結論 淋病奈瑟菌可引起龜頭化膿性包皮炎,該淋病奈瑟菌菌株多重耐藥并與其攜帶的耐藥基因密切相關。
龜頭包皮炎;淋病奈瑟菌;分離鑒定;耐藥性;耐藥基因
淋病奈瑟菌(Neisseriagonorrhoeae)俗稱淋球菌,是人類常見性傳播疾病淋病(gonorrhea)的病原體[1]。淋病是《中華人民共和國傳染病防治法》中重點防治的乙類傳染病,近年來其發病率一直占據我國性傳播疾病第2位[2]。早已肯定,淋病奈瑟菌引起人泌尿生殖道急性或慢性化膿性感染,新生兒經產道感染后引起淋球菌性結膜炎[3]。然而,我們從1例龜頭包皮炎患者龜頭膿包液中分離出淋病奈瑟菌,該菌株同時攜帶四環素耐藥相關tetM基因、β-內酰胺類抗生素耐藥相關TEM基因、紅霉素耐藥相關外排基因mefA和甲基化酶基因ermF基因,表現為對多種抗生素很強的耐藥性。
1 材料和方法
1.1 菌株來源及分離培養 龜頭包皮化膿性感染患者男性,33歲,無尿道刺激癥狀,2016年2月27日就診杭州某三甲醫院泌尿外科。無菌棉棒采取尿道分泌物及龜頭包皮膿包液標本,革蘭染色鏡檢并采用Mycoplasma IST 2試劑盒(梅里埃診斷產品有限公司)檢測支原體,然后將標本分別涂布淋病奈瑟菌巧克力選擇平板、哥倫比亞血平板、酵母菌鑒定平板,35 ℃、5% CO2培養24 h,觀察其生長情況及菌落形態。
1.2 菌株鑒定 挑取菌落革蘭染色鏡檢后用VITEK 2-compact型法國梅里埃VITEK 2-compact全自動細菌檢測分析系統及其配套的API-NH細菌鑒定卡進行鑒定[4]。此外,采用細菌基因組DNA提取試劑盒(Axygen)提取尿道口分泌物或龜頭膿包液、淋病奈瑟菌分離株DNA,紫外分光光度法檢測其純度和濃度。采用淋病奈瑟菌16S rRNA基因通用引物[5]、淋球菌核酸熒光PCR試劑盒(上海復星長征醫學科學有限公司)檢測上述DNA標本中淋病奈瑟菌16S rRNA基因片段。引物由上海Invitrogen公司合成,上游引物序列:5′-GCT ACG CAT ACC CGC GTT GC-3′, 下游引物序列:5′-CGA AGA CCT TCG AGC AGA CA-3′。PCR參數:94 ℃ 5 min;94 ℃ 30 s、55 ℃ 30 s、72 ℃ 1 min,35個循環;72 ℃ 10 min。采用溴乙錠預染色1.5%瓊脂糖凝膠電泳及Bio-Rad成像系統觀察260 bp目的擴增片段。
1.3 藥物敏感試驗 參照國內臨床通用的美國臨床實驗室標準化協會(CLSI)介紹的方法及判斷標準[5],采用K-B法檢測分離菌株對6種常見抗生素的敏感性。實驗中采用淋病奈瑟菌ATCC49981株為質控菌株。
1.4 β-內酰胺酶和超廣譜β-內酰胺酶確證試驗 分別采用顯色頭孢菌素法和雙紙片法進行β-內酰胺酶和超廣譜β-內酰胺酶(ESBLs)確證試驗[6-7]。淋病奈瑟菌分離株涂布于紙片頭孢硝噻吩紙片(BioMérieux)上,即刻觀察紙片顏色變化,若出現紅色表明該菌產β-內酰胺酶。淋病奈瑟菌分離株涂布于巧克力瓊脂(Oxoid)平板上,然后貼上頭孢他啶、頭孢他啶/克拉維酸、頭孢噻肟、頭孢噻肟/克拉維酸藥物紙片(Oxoid),37 ℃孵育24 h后觀察結果。若頭孢他啶/克拉維酸或頭孢噻肟/克拉維酸紙片抑菌環直徑較頭孢他啶或頭孢噻肟紙片抑菌環直徑≥5 cm,表明該菌株產ESBLs。實驗中以不產ESBLs大腸埃希菌ATCC25922株為陰性對照、產ESBLs肺炎克雷伯菌ATCC700603株為陽性對照。
1.5 耐藥基因檢測 按上法提取淋病奈瑟菌分離株DNA,紫外分光光度法檢測其純度和濃度[4]。采用文獻報道的引物以及Ex-Taq PCR試劑盒(TaKaRa)檢測上述DNA標本中TEM、tetM、ermF、mefA耐藥基因片段,反應參數同上[8-10]。引物并由上海Invitrogen公司合成,其序列(見表1)。
表1 淋病奈瑟菌耐藥基因PCR引物
Tab.1 Primers for amplification of drug resistance genes ofN.gonorrhoeae
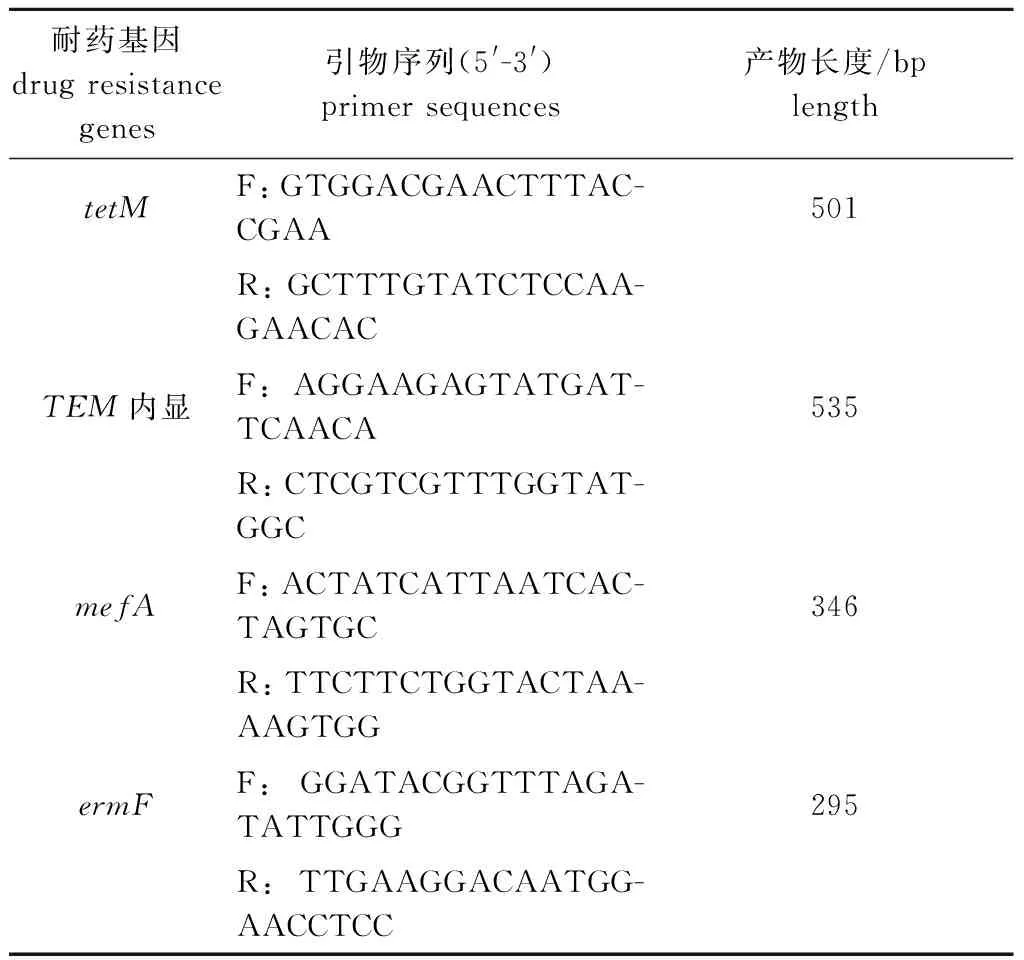
耐藥基因drugresistancegenes引物序列(5'-3')primersequences產物長度/bplengthtetMF:GTGGACGAACTTTAC-CGAA501R:GCTTTGTATCTCCAA-GAACACTEM內顯F:AGGAAGAGTATGAT-TCAACA535R:CTCGTCGTTTGGTAT-GGCmefAF:ACTATCATTAATCAC-TAGTGC346R:TTCTTCTGGTACTAA-AAGTGGermFF:GGATACGGTTTAGA-TATTGGG295R:TTGAAGGACAATGG-AACCTCC
F and R: upstream and downstream primers respectively
2 結 果
2.1 臨床標本檢查結果 龜頭膿包液中可見革蘭陰性雙球菌,部分雙球菌位于多形核白細胞內(圖1A),尿道分泌物未見細菌,但兩種標本支原體檢測結果均為陰性。尿道分泌物各種平板培養結果均為陰性,龜頭膿包液酵母菌鑒定平板培養結果陰性,但哥倫比亞血平板和淋病奈瑟菌選擇平板培養結果陽性,其菌落細小、凸起、光滑、圓形、灰白色,革蘭染色鏡檢為革蘭陰性雙球菌(圖1B)。淋病奈瑟菌16S rRNA基因PCR結果顯示,僅龜頭膿包液以及淋病奈瑟菌選擇平板上菌落檢出淋病奈瑟菌16S rRNA基因片段(圖2)。
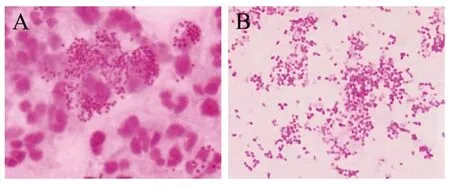
圖1 龜頭膿包液(A)及選擇平板上菌落(B)革蘭染色鏡檢結果(100×)Fig.1 Microscopic examination results of glans pustule (A) and colonies (B) on selective plate after Gram staining (100×)

M: DNA marker(TaKaRa); 1-3: PCR results for detecting urethral secretions,balanus pustule liquids and selective plates of N. gonorrhoeae 16S rRNA genes圖2 不同標本淋病奈瑟菌16S核糖體rRNA基因PCR檢測結果Fig.2 PCR results for detecting different samples of N. gonorrhoeae 16S rRNA gene
2.2 分離菌株生化反應鑒定結果 分離菌株經VITEK 2-compact全自動細菌檢測分析系統及其API-NH細菌鑒定卡鑒定為淋病奈瑟菌,鑒定值=99%,各生化反應中營養瓊脂35 ℃培養、硝酸鹽還原試驗NO3(red)、NO2→N2以及麥芽糖、乳糖、蔗糖、果糖發酵試驗結果均為陰性,但葡萄糖發酵試驗結果陽性。
2.3 藥敏試驗結果 淋病奈瑟菌分離株對青霉素G、環丙沙星、四環素、紅霉素耐藥,但對頭孢西丁、頭孢噻肟敏感(表2)。
表2 淋病奈瑟菌分離株藥敏試驗結果
Fig.2 Results of drug sensitive test of theN.gonorrhoeaeisolate

抗生素antibioticsKB值KBvalues折點范圍breakpoints結果判定results青霉素G(penicillinG)626-47耐藥drug-resistant環丙沙星(ciprofloxacin)627-41耐藥drug-resistant四環素(tetracycline)2430-38耐藥drug-resistant頭孢噻肟(cefotaxime)45>=31敏感drug-sensitive頭孢西丁(cefoxitin)3323-28敏感drug-sensitive
2.4 β-內酰胺酶及ESBLs確證試驗結果 淋病奈瑟菌分離株涂布的頭孢硝噻吩紙片由黃色轉變為紅色,表明該菌株產β-內酰胺酶。頭孢他啶對淋病奈瑟菌分離株抑菌環直徑18 mm、頭孢他啶/克拉維酸17 mm、頭孢噻肟32 mm、頭孢噻肟/克拉維酸35 mm。由于頭孢他啶/克拉維酸或頭孢噻肟/克拉維酸抑菌環直徑與頭孢他啶或頭孢噻肟抑菌環直徑之差小于5 mm,表明該菌株不產ESBLs。
2.5tetM、TEM、mefA、ermF基因PCR檢測結果 淋病奈瑟菌分離株四環素耐藥相關tetM基因、β-內酰胺酶TEM基因、紅霉素耐藥相關mefA和ermF基因PCR結果均為陽性(圖3)。
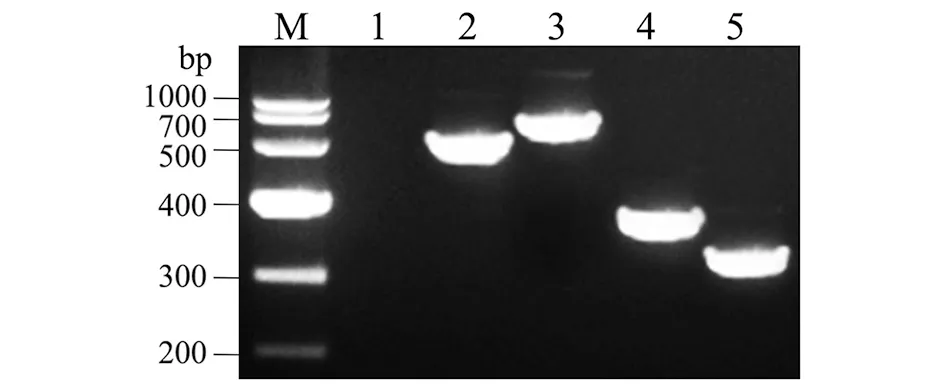
M: DNA marker(TaKaRa); 1: blank control; 2-5: PCR results of tetM,TEM,mefA and ermF genes of the N. gonorrhoeae isolate圖3 淋病奈瑟菌分離株tetM、TEM、mefA、ermF基因PCR檢測結果Fig.3 PCR results of tetM,TEM,mefA and ermF genes of the N. gonorrhoeae isolate
3 討 論
淋病是全球流行的人類性傳播疾病,臨床上主要表現為泌尿道化膿性炎癥,該菌雖可上行感染引起男性附睪炎、前列腺炎或引起女性陰道炎、子宮炎[11-13],但未有引起龜頭包皮炎的報道。因此,臨床上一般采集尿道分泌物檢測淋病奈瑟菌。本文中患者既無泌尿道化膿性炎癥的癥狀與體征,其尿道分泌物中也未分離出淋病奈瑟菌或檢出該菌16S rDNA基因片段,但在龜頭包皮膿包液中不僅分離出淋病奈瑟菌,也檢出了該菌16S rDNA基因,表明該患者為淋球菌龜頭包皮炎。
近年來淋病奈瑟菌臨床分離株對抗生素、尤其是對環丙沙星、青霉素、四環素等臨床一線抗菌藥物的耐藥性日趨增強[14]。了解淋病奈瑟菌臨床菌株的耐藥譜、耐藥基因型及其相互關系,不僅可指導臨床合理用藥,同時也有助于進一步揭示耐藥表型與基因型關系并為開發新的抗菌藥物提供依據。
青霉素類抗生素能與本質為細菌細胞壁肽聚糖合成相關內肽酶和羧肽酶的青霉素結合蛋白(penicilin-binding proteins,PBPs)結合,導致酶分子變構失活,細菌因細胞壁缺陷而裂解[2]。TEM基因產物β-內酰胺酶可水解青霉素類抗生素,故攜帶TEM基因細菌表現為對青霉素耐藥[15]。環丙沙星是大環內酯類抗生素。mef基因產物為細菌排出環丙沙星等大環內酯類抗生素的外排蛋白,erm基因產物為rRNA甲基化酶,該酶可使大環內酯類抗生素作用靶位核糖體50S亞基發生改變,降低大環內酯類藥物結合能力而導致耐藥[16]。四環素類抗生素主要通過與細菌核糖體30S亞基結合,抑制氨基酰-tRNA與核糖體結合而阻斷細菌蛋白合成[17]。tetM基因產物為核糖體保護蛋白,可對抗四環素類抗生素阻斷氨基酰-tRNA與核糖體結合的作用,從而使細菌產生對四環素類抗生素的耐藥性[18]。我們的藥物敏感試驗結果顯示,淋病奈瑟菌分離株對青霉素G、環丙沙星、四環素耐藥,但對頭孢噻肟和頭孢西丁敏感;β-內酰胺酶和ESBLs確證試驗結果顯示,淋病奈瑟菌分離株產β-內酰胺酶,但不產ESBLs。我們的PCR檢測結果顯示,淋病奈瑟菌分離株具有TEM、tetM、mef和erm基因,與該菌株耐藥譜及其表型相符。
[1] Sunita G,Sarika A,Shreekant V,et al. Rice and Sanjay Ram Properdin is critical for antibody-dependent bactericidal activity againstNeisseriagonorrhoeaethat recruit C4b-binding protein[J]. J Immunol,2012,188(7): 3416-3425. DOI: 10.4049/jimmunol. 1102746
[2] Gong XD,Yue XL,Jiang N,et al. Epidemiological characteristics and trends of gonorrhea in China from 2000 to 2014[J]. Chin J Dermatol,2015,48(5): 301-306. DOI: 10.3760/cma.j.
issn.0412-4030.2015.05.002
[3] Yan J. Medical microbiology[M]. 3rd Edition,Beijing: The High Education Publication House,China,2016: 25-26,82-84. (in Chinese)
[4] Dong HL,Guo YY,Mao JF,et al. Analysis on the results of main sexually transmitted diseases tested in 6 682 male cases suspected with genitourinary infection[J]. Chin J Zoonoses,2014,30(1): 102-105. DOI: 10.3969/cjz.j.issn.1002-2694.2014.01.022
[5] David J,Farrel L. Evaluation of amplicorNeisseriagonorrhoeaePCR using cppB nested PCR and 16S rRNA PCR[J]. J Clin Microbiol,1999,37(2): 386-390. DOI: 0095-1137/99 /04.0010
[6] Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing[S]. Twenty-fourth Informational Supplement. CLSI document M100-S24. Wayne: Clinical and Laboratory Standards Institute. 2014.
[7] Laura M,Valerie C,Zaelle D,et al. FirstNeisseriagonorrhoeaegenotyping analysis in France: identification of a strain cluster with reduced susceptibility to ceftriaxone[J]. J Clin Microbiol,2009,47(11): 3540-3545. DOI: 10.1128/JCM.01236-09
[8] Joseph RD,Lalitagauri MD,Douglas JB,et al. Evolution and dissemination of extended spectrum β-lactamase-producingKlebsiellapneumoniae: Epidemiology and molecular report from the SENTRY Antimicrobial Surveillance Program (1997-2003)[J]. Diagn Microbiol Infect Dis,2005,51(1): 1-7. DOI: 10.1016/j.diagmicrobio.2004.08.001
[9] Chunxin W,Peiquan C,Dong C,et al. APseudomonasaeruginosaisolate producing the GES-5 extended-spectrum β-lactamase[J]. J Antimicrob Chemoth,2006,57(6): 1261-1262. DOI: 10.1093/jac/dkl116
[10] Li GM,Chen Qun,Chen JJ,et al. Resistance genes of multi-drug resistance strains ofNeisseriagonorrhoeae[J].Chin J Nosocomiol Vol,2005,15(8): 852-854. DOI: 10.3321/j.issn:1005-4529.2005.08.004
[11] Ros CTD,Schmitt CDS. Global epidemiology of sexually transmitted diseases[J]. Lancet,2008,10(1): 110-114. DOI: 10.1111/j.1745-7262.2008.00367
[12] Johnson MB,Criss AK. Resistance ofNeisseriagonorrhoeaeto neutrophils[J]. Front Microbiol,2011,2(1): 77-77. DOI: 10.3389/fmicb.2011.00077
[13] Yin F,Feng Z,Li X. Spatial analysis of county-based gonorrhoea incidence in mainland China from 2004 to 2009[J]. Sex Health,2012,9(3): 227-232. DOI: 10.1071/SH11052
[14] Unemo M,Nicholas RA. Emergence of multi-drug resistant,extensively drug-resistant and untreatable gonorrhea[J]. Future Microbiol,2012,7(12): 1401-1422. DOI: 10.2217/ fmb.12.117
[15] Unemo M,Shafer WM. Antimicrobial resistance inNeisseriagonorrhoeaein the 21st century: past,evolution and future[J]. Clin Microbiol Rev,2014,27(3): 587-613. DOI: 10.1128/CMR.00010-14[16] Luna VA,Cousin S,Whittington WLH,et al. Identification of the conjugative mef gene in clinicalAcinetobacterjuniiandNeisseriagonorrhoeaeisolates[J]. Antimicrob Agents CH,2000,44(9): 2503-2506. DOI: 10.1128/AAC.44.9.2503-2506.2000
[17] Flrez AB,Ammor MS,Martín PL,et al. Molecular analysis of tet(W) gene-mediated tetracycline resistance in dominant intestinal bifidobacterium species from healthy humans[J]. Appl Environ Microb,2006,72(11): 7377-7379. DOI: 10.1128/AEM.00486-06
[18] Li YW,Shi ZQ,Zhao PL,et al. The research on plasmid profiles of TEM-1 encoding gene in penicillinase-producingNeisseriagonorrhoeaeandtetMgene in high level tetracycline-resistantNeisseriagonorrhoeaein Fosha[J]. Chin J Antibiot,2014,39(3): 236-239. DOI: 10.3969/j.issn.1001-8689.2014.03.016
Isolation and identification ofNeisseriagonorrhoeaestrain from a balanoposthitis patient and drug resistance mechanism of the isolate
GE Yu-mei,HU Qing-feng,ZHU Yong-ze,ZHOU Yong-lie,LYU Huo-yang
(ZhejiangProvincialPeople’sHospital,Hangzhou310014,China)
We isolated and identified the bacterial pathogen in a pyogenic balanoposthitis patient and investigated the drug resistance and its mechanism of the isolate. Urethral secretions and balanus pustule liquids were collected for microscopic examination after Gram-staining and detection of mycoplasma usingMycoplasmaIST 2 kit. The two samples were inoculated on Columbia blood plate,N.gonorrhoeaeselective plate and chromID Candida plate for isolation. The obtained colonies were identified by VITEK 2-compact automatic bacterial detection and analysis system. Moreover,PCR was performed to detect 16S rRNA gene ofN.gonorrhoeaein the samples and colonies. KB method was applied for detecting susceptibility of five common antibiotics against the isolate. The β-lactamase and extended spectrum β-lactamase confirmatory tests were used to investigate the enzyme production of the isolate as well as drug resistance-associated tetM,TEM,mefA and ermF genes in the isolate were detected by PCR. Results showed that all the clinic samples showed negative for mycoplasma. All the isolating cultivation results of urethral secretions were negative while the balanus pustule liquids provided positive isolating cultivation in the blood and selective plates. The VITEK 2-compact system and 16S rRNA-PCR revealed that the isolated strain belongs toN.gonorrhoeae. The isolate can produce β-lactamases and resist to penicillin G,ciprofloxacin and tetracycline. The tetM,TEM,mefA and ermF genes could be found in the isolate’s genome. The patient’s balanoposthitis is caused by infection ofN.gonorrhoeae. The multidrug resistance ofNeisseriagonorrhoeaeisolate is closely associated with its carried resistant genes.
balanoposthitis;Neisseriagonorrhoeae; isolation and identification; drug resistance; resistance gene
Lyu Huo-yang,Email: geyumei1990@hotmail.com
10.3969/j.issn.1002-2694.2017.05.009
浙江省醫藥衛生科技計劃項目(2017KY004)資助
呂火烊,geyumei1990@hotmail.com
浙江省人民醫院檢驗中心,杭州 310014
R378.1
A
1002-2694(2017)05-0432-04
2016-11-14 編輯:劉岱偉
Supported by the Medical Scientific Research Foundation of Zhejiang Province (No. 2017KY004)
猜你喜歡
保健醫苑(2022年5期)2022-06-10 07:46:38
現代臨床醫學(2022年3期)2022-06-06 07:59:40
昆明醫科大學學報(2022年1期)2022-02-28 07:43:40
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2020年12期)2021-01-18 06:57:46
中學生數理化·七年級數學人教版(2020年12期)2021-01-18 06:57:46
科學大眾(2020年12期)2020-08-13 03:22:22
海峽科技與產業(2016年3期)2016-05-17 04:32:12