濰坊社區65歲以上老年人高尿酸血癥患病率及影響因素分析
2017-03-01 13:43:55阮玉鳳
上海醫藥 2017年2期
阮玉鳳
摘 要 目的:調查本社區65歲以上老年人高尿酸血癥(HUA)的患病情況,并對其相關危險因素進行分析。方法:選擇2015年4—10月在本社區進行體檢的2 433例65歲以上老年人,進行問卷調查、體格檢查及實驗室檢查。根據血尿酸水平分為HUA組290例和正常尿酸組2 143例,采用非條件Logistics回歸分析HUA的影響因素。結果:2 433例受檢者中,HUA患病率為11.92%,男性和女性患病率分別為18.58%和6.77%(P=0.000),HUA組男性比例、平均年齡、高血壓患者比例、BMI、血肌酐、尿素、γ-谷氨酰轉肽酶、總蛋白、白蛋白、TG水平均較正常尿酸組升高,而HDL水平較正常尿酸組明顯下降(P<0.05),多因素Logistics回歸分析顯示超重、腎功能下降、γ-谷氨酰轉肽酶升高、白蛋白升高、高TG血癥為HUA的危險因素(P<0.05)。結論:該社區65歲以上老年人HUA患病率相對不高,超重、腎功能下降、高TG血癥可能是發生HUA的危險因素,應采取相應措施進行預防。
關鍵詞 高尿酸血癥;患病率;危險因素
中圖分類號:R589.7 文獻標志碼:A 文章編號:1006-1533(2017)02-0035-03
Analysis of the incidence of hyperuricemia in the elderly people over 65 years old in Weifang Community and its influencing factors
RUAN Yufeng
(Weifang Community Health Service Center of Pudong New District, Shanghai 200122, China.)
ABSTRACT Objective: To investigate the prevalence of hyperuricemia(HUA)among the community residents over 65 years old in this community and analyze the related risk factors. Methods: A total of 2 433 elderly people over 65 years old were selected from April to Oct. 2015 who had the health check in this community and investigated with the questionnaire and had the health examination and biochemical tests. According to the levels of HUA, they were divided into a HUA group and a normal uric acid group. The non conditional logistic regression analysis was used to analyze the influencing factors of HUA. Results: Of 2 433 examined subjects, the total incidence of HUA was 11.92%, and the prevalence of male and female was 18.58% and 6.77%, respectively(P=0.000). The male ratio, the average age, the proportion of patients with hypertension, BMI, serum creatinine, urea,γ-alanine aminotransferase(γGT), total protein, albumin, and triglyceride(TG)levels in the HUA group were higher than those in the normal uric acid group, but high-density lipoprotein(HDL)level was significantly lower in the HUA group than that in the normal uric acid group(P<0.05). Multi factor Logistics regression analysis showed that overweight, renal function decline, γGT, elevated albumin, and high TG were the risk factors of HUA(P<0.05) . Conclusion: The prevalence rate of HUA is relatively low in the elderly people over 65 years old in this community. The overweight, kidney function decline and high TG levels may be the risk factors of HUA, and corresponding measures should be taken for prevention.
KEY WORDS hyperuricemia; prevalence; risk factor
高尿酸血癥(HUA)是一種嘌呤代謝障礙性疾病,隨著人民生活水平的提高,HUA的患病率呈逐年上升趨勢,特別是在經濟發達的城市和沿海地區,HUA的患病率達5%~23.5%[1-2],接近西方發達國家的水平[3]。HUA不僅與痛風的發生密切相關,也與很多疾病的發生有相關性,如高血壓、糖尿病、心血管疾病和慢性腎臟病等[4]。本研究旨在了解本社區65歲以上老年人群HUA的患病情況以及發生HUA的危險因素,從而為臨床中防治HUA提供依據。
1 資料與方法
1 . 1 研究對象
2015年4~10月在我院健康家園參加體檢的65歲以上老年人2 433例,年齡65~96歲,其中男性1 060例,年齡(74.02±6.223)歲,女性1 373例,年齡(73.76±6.323)歲。考慮更年期后女性血尿酸水平接近男性,將血尿酸水平高于420 μmol/L定義為高尿酸血癥,根據入選者血尿酸水平分為HUA組290例,其中男性197例,女性93例,血尿酸正常組2 143例,其中男性863例,女性1 280例。
1 . 2 方法
資料收集:調查員經過統一培訓,并考核合格。根據居民健康檔案收集研究對象的一般狀況,包括有無高血壓、糖尿病,由有經驗的醫護人員采用統一的檢查工具,測量入院者的身高、體重,計算體重指數(BMI),并記錄在健康體檢表上。
實驗室檢查:受檢者禁食12 h,抽取肘靜脈血5 ml,采用日立7 100全自動生化儀檢測尿酸、空腹血糖、肝、腎功能、血脂等指標。
1 . 3 統計學方法
2 結果
2 . 1 總體患病情況
2 433例調查對象中共290例HUA患者,HUA患病率為11.92%,其中男性197例,患病率為18.58%,女性93例,患病率6.77%,男性HUA的患病率要高于女性,差異有統計學意義(χ2=79.488,P=0.000),HUA組平均年齡要高于血尿酸正常組(74.97±6.449比73.72±6.243),差異有統計學意義(P=0.001)。
2 . 2 HUA發生的相關影響因素分析
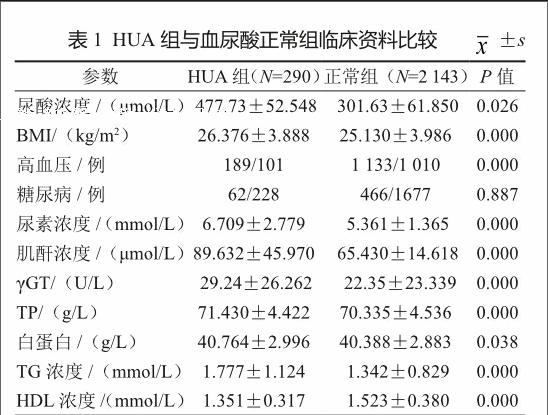
2.2.1 合并疾病比較
HUA組BMI、高血壓發生率、糖尿病發生率、尿素、肌酐、γ-谷氨酰轉肽酶(γGT)、總蛋白(TP)、白蛋白、甘油三酯(TG)水平均高于尿酸正常組,而高密度脂蛋白(HDL)水平低于血尿酸正常組(表1)。
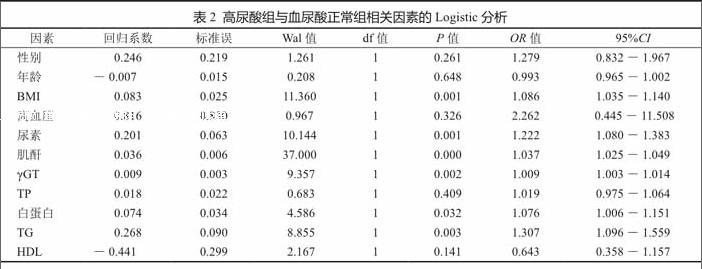
2.2.2 HUA相關影響因素的多因素Logistics回歸分析
以年齡、性別、BMI、是否有高血壓、尿素、肌酐、γGT、總蛋白、白蛋白、TG、HDL白為自變量,以HUA為因變量進行多因素Logistics回歸分析,結果顯示高BMI、高尿素水平、高肌酐水平、高γGT水平、高白蛋白水平以及高TG血癥是HUA的危險因素(P<0.05,表2)。
3 討論
HUA的流行總體呈現逐年升高的趨勢,男性高于女性,且有一定的地區差異,南方和沿海經濟發達地區較同期國內其他地區患病率高,可能與該地區居民攝入過多高嘌呤的海產品、動物內臟、肉類食品以及大量飲用啤酒等因素有關[1]。本研究顯示本社區65歲以上老年人HUA患病率為11.92%,明顯低于屈炯堂等[5]對中山市老年退休人員HUA患病率的調查,他們的患病率為29.21%,可能與本社區居民健康意識的提高有一定關系。本研究還發現男性HUA的患病率顯著高于女性,與大多研究均一致,究其原因,可能與男女生活和飲食方式的不同有關。此外,研究還發現,年齡與HUA的發生也有一定關系,HUA組平均年齡顯著高于血尿酸正常組,說明年齡也是發生高尿酸血癥的一個危險因素。
當研究肝、腎功能、血脂等指標與HUA的關系時發現血尿素、肌酐、γGT、總蛋白、白蛋白、TG水平升高以及HDL水平下降是HUA發生的危險因素,進一步的多因素Logistics回歸分析顯示BMI、尿素、肌酐、γGT、白蛋白、TG水平升高是HUA發生的危險因素。HUA與腎功能水平下降互為因果關系:HUA水平升高可導致急性尿酸性腎病、慢性尿酸性腎病和腎結石,增加發生腎功能衰竭的風險。而腎功能不全又是痛風的重要危險因素。大量研究證實,隨著HUA的增高,慢性腎病(CKD)[6]、糖尿病腎病的患病率顯著增加[7];而且,HUA也是急慢性腎功能衰竭發生[8]及預后差[9]的強有力的預測因素。降低HUA對腎臟疾病的控制有益[10]。在日本,對于慢性腎臟病3級以上的患者,常規治療方案推薦使用別嘌呤醇及苯溴馬隆,通過降尿酸治療延緩CKD進展[11]。此外,本研究還發現HUA組TG水平較高,而HDL水平較低,進一步Logistics回歸分析顯示高TG是HUA發生的獨立危險因素,與國內多位學者的研究結果一致[5,12]。
許多研究發現高血壓、糖尿病、肥胖與HUA相關[13],甚至認為它們是HUA的危險因素。我們的分析顯示只有高血壓、高BMI與HUA的發生有關,進一步Logistics回歸分析顯示高BMI是HUA發生的獨立危險因素,造成研究結果差異的原因可能與研究人群的不同有一定關系。
總之,老年人群HUA患者應采取綜合防治措施,一方面,全科醫生應加強HUA的健康教育宣傳,同時對HUA患者進行飲食指導,重視尿酸以及相應代謝指標的測定,做到早期發現、及時治療與干預,在保護腎功能的同時,治療高尿酸血癥及伴發的相關疾病。
綜上所述,本研究分析本社區65歲以上體檢老年人HUA的患病率以及影響HUA的因素,鑒于橫斷面研究的局限性,其影響有待于進一步研究。此外,本研究未考慮部分入選者服用治療藥物對檢測結果的影響,故結論存在一定局限性。
參考文獻
[1] 閻勝利, 趙世華, 李長貴, 等. 山東沿海居民高尿酸血癥及痛風五年隨訪研究[J]. 中華內分泌代謝雜志, 2011, 27(7): 548-552.
[2] 周戈, 齊慧, 趙根明, 等. 上海市浦東新區居民高尿酸血癥與慢性腎病相關性研究[J]. 中華流行病學雜志, 2012, 33(4): 351-355.
[3] Luk AJ, Simkin PA. Epidemiology of hyperuricemia and gout[J]. Am J Manag Care, 2005, 11(11): 465-468.
[4] Yang T, Ding X, Wang YL, et al. Association between high-sensitivity C-reactive protein and hyperuricemia[J]. Rheumatol Int, 2016, 36(4): 561-566.
[5] 屈炯堂, 劉本堅, 梁美玲. 老年退休人員高尿酸血癥的患病率及影響因素分析[J]. 中華老年心腦血管雜志, 2013, 15(11): 1142-1145.
[6] Kawashima M, Wada K, Oht H, et al. Association between asymptomatic hyperuricemia and new-onset chronic kidney disease in Japanese male workers: a long-term retrospective cohort study[J]. BMC Nephrology, 2011, 12(31): 1186/1471-2369.
[7] Cai XL, Han XY, Ji LN. High-normal serum uric acid is associated with albuminuria and impaired glomerular filtration rate in Chinese type 2 diabetic patients[J]. Chin Med J, 2011, 124(22): 3629-3634.
[8] Ben-Dov IZ, Kark JD. Serum uric acid is a GFR-independent long-term predictor of acute and chronic renal insufficiency: the Jerusalem lipid research clinic cohort study[J]. Nephrol Dial Transplant, 2011, 26(8): 2558-2566.
[9] Murea M. Advanced kidney failure and hyperuricemia[J]. Adv Chronic Kidney Dis, 2012, 19(6): 419-424.
[10] Siu YP, Leung KT, Tong MK, et al. Use of allopurinol in slowing the progression of renal disease through its ability to lower serum uric acid level[J]. Am J Kidney Dis, 2006, 47(1): 51-59.
[11] Nakaya I, Namikoshi T, Tsuruta Y, et al. Management of asymptomatic hyperuricaemia in patients with chronic kidney disease by Japanese nephrologists: a questionnaire survey[J]. Nephrology(Carlton), 2011, 16(5): 518-521.
[12] 宋薇, 劉精東, 陳志雄, 等. 南昌地區40歲以上社區居民高尿酸血癥和痛風的患病率調查及相關影響因素分析[J].中國全科醫學雜志, 2014, 17(2): 181-183.
[13] Poletto J, Harima HA, Roberta SR, et al. Hyperuricemia and associated factors: a cross-sectional study of JapaneseBrazilians[J]. Cad Saude Publica, 2011, 27(2): 369-378.
[14] Jia Z, Zhang X, Kang S, et al. Serum uric acid levels and incidence of impaired fasting glucose and type 2 diabetes mellitus: A meta-analysis of cohort studies[J]. Diabetes Res Clin Pract, 2013, 101(1): 88-96.
[15] Cannon PJ, Stason WB, Demartini FE, et al. Hyperuricemia in primary and renal hypertension[J]. N Engl J Med, 1966, 275(9): 457-464.
猜你喜歡
健康體檢與管理(2022年2期)2022-04-15 22:33:17
昆明醫科大學學報(2021年1期)2021-02-07 01:06:44
今日健康(2016年12期)2016-11-17 14:41:50
今日健康(2016年12期)2016-11-17 13:12:34
今日健康(2016年12期)2016-11-17 12:29:29
科技資訊(2016年19期)2016-11-15 10:33:36
中國實用醫藥(2016年24期)2016-10-17 05:32:48
養生保健指南(2016年4期)2016-03-22 12:25:57
中國男科學雜志(2016年9期)2016-03-20 15:00:09
中國健康心理學雜志(2015年5期)2015-09-05 09:55:52
