Who needs further evaluations to diagnose upper urinary tract urothelial cancers among patients with abnormal findings by enhanced CT?
2016-04-27 06:06:51AkioTkyngiAtsushiTkhshiFumimsFukutMnbuOkdMshiroMtsukiShunsukeStoTeruhisUehrShuichiKtoYoshioTkgi
Asian Journal of Urology 2016年1期
Akio Tkyngi*,Atsushi Tkhshi,Fumims Fukut Mnbu OkdMshiro MtsukiShunsuke Sto Teruhis UehrShuichi KtoYoshio Tkgi
aDepartment of Urology,Hakodate Goryoukaku Hospital,Hakodate,Hokkaido,Japan
bDepartment of Urology,Sapporo Medical University School of Medicine,Sapporo,Hokkaido,Japan
Who needs further evaluations to diagnose upper urinary tract urothelial cancers among patients with abnormal findings by enhanced CT?
Akio Takayanagia,b,*,Atsushi Takahashia,Fumimasa Fukutaa,b, Manabu Okadaa,b,Masahiro Matsukia,b,Shunsuke Satoa,b, Teruhisa Ueharaa,b,Shuichi Katoa,b,Yoshio Takagia
aDepartment of Urology,Hakodate Goryoukaku Hospital,Hakodate,Hokkaido,Japan
bDepartment of Urology,Sapporo Medical University School of Medicine,Sapporo,Hokkaido,Japan
Upper urinary tract
urothelial cancers;
Enhanced CT;
Ureteroscopy;
Retrograde
pyelography
Objective:We evaluated who would need further evaluations such as retrograde pyelography(RP)and/or ureteroscopy to diagnose upper urinary tract urothelial cancers (UUTUCs)when abnormal findings for the upper urinary tract(UUT)were detected by enhanced computed tomography(CT).
Methods:We retrospectively analyzed 125 patients who underwent enhanced CT for various reasons and had abnormal findings for the UUT.Patients whose tumors were suspected to be of extraureteral origin were excluded.All patients received RP and/or ureteroscopy to evaluate the UUTUCs.
Results:The median age of the 125 patients was 70 years and gross hematuria(26.4%)was the most frequently observed symptoms.RP,ureteroscopy and both were performed for 121,59 and 55 patients,respectively.CT revealed tumor-like lesions in 58 patients and the other patients had non-tumor-like lesions.UUTUCs were found in 43(34.4%)of the 125 patients.All of them had tumor-like lesions on CT.In 58 patients who had tumor-like lesions on CT,univariate and multivariate analyses revealed that tumor diameter and tumor enhancement were significant predictive factors for UUTUCs.ROC curve analysis of enhanced CT to diagnose UUTUCs revealed that a tumor diameter of 18 mm was the best cutoff point.The sensitivity,specificity and accuracy were 90.0%,98.8%and 92.7%for RP and 95.5%,100%and 97.1%for ureteroscopy, respectively.Both of them had high sensitivity,specificity and accuracy.
Conclusion:We should decide to evaluate the UUT according to the tumor diameter on enhanced CT.When we evaluate the UUT in patients with tumor diameters of less than 20 mm,ureteroscopy is recommended.
?2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
1.Introduction
Upper urinary tract urothelial cancers(UUTUCs)are rare, accounting for approximately 5%-10%of all urothelial carcinomas[1].We conventionally perform retrograde pyelography(RP)and/or ureteroscopy for diagnosis when UUTUC is suspected based on computed tomography(CT), intravenous urography and so on.
Recently,thanks to the development of high resolution CT,diagnostic accuracy has improved not only for urological cancers,but also for other malignancies[2-5].We can diagnose some cases as UUTUCs by CT findings alone[6], although other cases may require RP and/or ureteroscopy to determine whether the abnormal lesion detected by CT or another modality is UUTUC or not.Unfortunately,we do not know which patients with abnormal lesions found by CT need further evaluation including RP and/or ureteroscopy for diagnosis of UUTUCs.In this study,we retrospectively analyzed patients who had abnormal findings detected by enhanced CT and subsequently underwent RP and/or ureteroscopy,and evaluated who needs such further invasive evaluations to diagnose UUTUCs.
2.Materials and methods
2.1.Patients
We retrospectively analyzed 125 patients who underwent enhanced CT for various reasons and had abnormal UUTfindings between January 2006 and December 2010. Abnormal UUT findings included tumor-like lesions in the UUT,hydronephrosis and hydroureter.These patients received further evaluation,including RP and/or ureteroscopy to evaluate the UUT.Enhanced CT in the early phase was basically performed for these patients using a 64-multidetector row scanner(Toshiba Medical Systems,Tokyo, Japan).We excluded patients whose tumors were suspected to be of extraureteral origin.One of the two chief physicians (AT and YT)made the final decision to perform RP,ureteroscopy or both of them.Tumor enhancement was defined as a change of the CT value of 10 HU or more.This study was approved by the ethic committee of Hakodate Goryoukaku Hospital(#H2801).
2.2.Methods of retrograde pyelography
RP was performed under anesthesia for males but without it for females.A 6 Fr open-ended catheter was inserted into the ureteral orifice using cystoscopy.Then contrast medium could be introduced directly into the upper collecting system and the ureters[7].We also obtained urine from the catheter for urine cytology.
2.3.Methods of ureteroscopy
Ureteroscopy was performed under anesthesia for all patients.A semi-rigid ureteroscope(6.9 Fr,MR-6LA,Olympus, USA)was inserted through the ureteral orifice and we examined the entire ureter[8].We have used a flexible ureteroscope(5.3 Fr,URF-P5,Olympus,Japan)in our hospital since 2008.Patients underwent both semi-rigid and flexible ureteroscopy from 2008 or later if a tumor above the ureteropelvic junction was suspected.
2.4.Follow-up of patients
All patients who were diagnosed with UUTUCs had received radical treatment or systemic therapy according to the clinical stage of the UUTUC.Patients who were diagnosed as not having UUTUC were generally followed up in our department every 3 months for at least 1 year.During follow-up UUTUCs were not detected in any of these patients.
2.5.Statistical analysis
Statistical analyses were performed with EZR(Saitama Medical Center,Jichi Medical University,Japan),which is a graphical user interface for R(The R Foundation for Statistical Computing).More precisely,it is a modified version of R commander designed to add statistical functions frequently used in biostatics[9].p<0.05 was considered to be significant.Univariate analysis was performed using the Mann-Whitney U test,chi-square test and log-rank test. Multivariate analysis was performed using Logistic regression analysis.We performed receiver operating characteristic(ROC)curve analysis to evaluate the diagnostic ability of enhanced CT and calculated the area under the curve (AUC).To determine the cutoff value for diagnosis,we used Youden’s Index(sensitivity+specificity-1)[10].
3.Results
3.1.Patients’characteristics
A total of 125 patients were eligible for this study.The median age of the patients was 70 years(Table 1).Gross hematuria was found in 33 patients(26.4%)and was the most frequently observed symptom.Fifty-seven(45.6%) patients were referred from other hospitals because ofabnormal UUT findings.Most of them underwent CTwithout having urinary tract symptoms and the details of why they did so were not clear.Although 58 patients had tumor-like lesions on CT,67 exhibited hydronephrosis or hydroureter without a tumor-like lesion.RP,ureteroscopy and both were performed in 121,59 and 55 patients,respectively. Sixteen patients underwent semi-rigid ureteroscopy before 2008,and the other 43 flexible ureteroscopy from 2008 or later.

Table 1Patients’characteristics.
3.2.Results of UUT evaluation
UUTUCs were found in 43(34.4%)of the 125 patients, ureteral stricture in 35(28.0%),ureteropelvic junction obstruction in 18(14.4%)and there were no abnormalfindings in 29(23.2%).Of the 58 patients with tumor-like lesions revealed by CT,43(74.1%)were finally diagnosed with UUTUCs.On the other hand,none of the 67 patients who did not show tumor-like lesions on CT were finally diagnosed with UUTUCs.Therefore the diagnostic accuracy of enhanced CT for UUTUCs was 88.0%.
3.3.Relationship between the CT findings and final diagnosis
We focused on the 58 patients with tumor-like lesions revealed by CT and evaluated the relationship between the tumor diameter in the axial plane and the final diagnosis (Fig.1).All 15 patients who had tumors with a diameter of 20 mmormore were finally diagnosed with UUTUCs.Of the 43 patients who had tumors with a diameter of less than 20 mm, 28(65.1%)patients were finally diagnosed with UUTUCs.
We performed statistical analysis of these 58 patients with tumor-like lesions revealed by CT to identify the predictive factors for UUTUCs using the following four factors:tumor diameter,the existence of hydronephrosis, enhancement of the tumor and tumor location.In univariate analysis,tumor diameter and tumor enhancement were significant predictive factors for UUTUCs(p=0.02, p=0.004)(Table 2).In multivariate analysis,tumor diameter and tumor enhancement remained significant(HR =1.23,p=0.01;HR=6.78,p=0.02,respectively).
We performed ROC curve analysis evaluating the diagnostic ability of enhanced CT using the tumor diameter (Fig.2).The AUC was 0.783 and the 95%confidence interval (95%CI)ranged from 0.641 to 0.925.The best cutoff point according to Youden’s Index was 18 mm and the sensitivity and specificity were 90.7%and 53.3%,respectively.
3.4.Results of retrograde pyelography
Of the 121 patients who underwent RP,36(29.8%)werefinally diagnosed with UUTUCs.False negative results were found in four(3.3%)patients and a false positive result in one(0.8%).Three of the four patients with false negatives underwent ureteroscopy and UUTUCs were detected. Although the other patient underwent semi-rigid ureteroscopy,UUTUC was not detected.Because his urine cytology obtained during ureteroscopy was positive,he was finally judged as having UUTUC based on the positive urine cytology.Thereafter he underwent radical nephroureterectomy and pathological examination confirmed UUTUC in his renal pelvis.The patient with the false positive result underwent ureteroscopy and was diagnosed as having multiple ureteral polyps.The sensitivity,specificity,and accuracy of RP in the 121 patients were 90.0%,98.8%,and 95.9%,respectively(Table 3).On the other hand,in 58 of the 121 patients with tumor-like lesions on CT,the accuracy of RP was 92.7%(Table 4).
3.5.Results of ureteroscopy
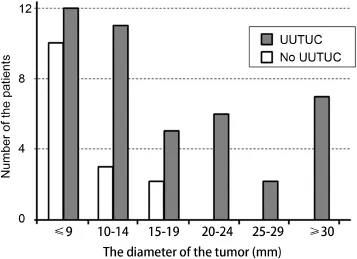
Figure 1The relationship between the CT findings and thefinal diagnosis.UUTUC,upper urinary tract urothelial cancer.
Of the 59 patients who underwent ureteroscopy,21(35.6%) were finally diagnosed with UUTUCs.Although a falsenegative result was found in one(1.7%)patient,there was no false positive result.The renal pelvic cancer of this patient,who was described in the“results of RP”,was missed because we could use only a semi-rigid ureteroscope at that time.There were no severe adverse events due to RP or ureteroscopy in any case.The sensitivity,specificity, and accuracy of ureteroscopy in the 59 patients were 95.5%,100%,and 98.3%,respectively(Table 3).On the other hand,in the 58 patients with tumor-like lesions revealed by CT,the accuracy of ureteroscopy was 97.1% (Table 4).

Table 2Univariate and multivariate analyses for risk factors to predict UUTUC in 58 patients.
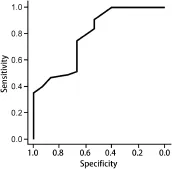
Figure 2ROC curve analysis to evaluate the diagnostic ability of enhanced CT.ROC,receiver operating characteristic; CT,computed tomography.
4.Discussion
Enhanced CT is widely performed to examine the UUT.In this study we focused on 125 patients who showed abnormal findings in the UUT by enhanced CT.Our results showed that the diagnostic accuracy of enhanced CT was as high as 88.0%.Therefore contrast CT is assumed to be very useful to examine the UUT.Caoili et al.[11]and Maheshwari et al.[12]also reported that CT was useful to examine the UUT,and its sensitivity was 89%-100%.
In our study,74.1%of the patients with tumor-like lesions found by enhanced CT were finally diagnosed with UUTUCs.According to the results of ROC curve analysis,a tumor diameter of 18 mm was the best cutoff point to detect UUTUCs.However,9.3%of the patients were false negative,and 18 mm is a little complicated to use in the clinical setting.To reduce the false negative rate and enhance the power of UUTUC screening by CT,we believe 20 mm was the best cutoff point.Although we had a limited number of patients,all the patients with tumor diameters of 20 mm or more had UUTUCs.
In this study,we had false-negative findings in three examined by RP(diagnostic accuracy:92.5%)and one patient examined by ureteroscopy(diagnostic accuracy: 96.7%).The one false-negative patient examined by semirigid ureteroscopy had renal pelvic cancer.At that time we could not use a flexible ureteroscope.Had flexible ureteroscopy been possible,we might have been able to detect the tumor.Both RP and ureteroscopy had high sensitivity and specificity to evaluated the UUTUCs.Since ureteroscopy,especially the flexible type,might be consider desirable to evaluate UUT.It had higher accuracy to diagnose UUTUCs compared to RP,unfortunately there was no statistical difference(p=0.665),since there may be patient’s selection bias(discussed below).
Based on our results,we propose an algorithm to evaluate the UUT(Fig.3).To examine the UUT,it is desirable to perform enhanced CT.If tumor-like lesions are detected byCT,we should consider the necessity of further evaluation according to the tumor diameter.If it is 20 mm or greater in addition to tumor enhancement,we can judge the tumor to be UUTUC.On the other hand,if the tumor diameter is less than 20 mm,we should perform further ureteroscopic evaluation of the UUT.Otherwise,if tumor-like lesion were not detected by CT,we may not need to recommend performing ureteroscopy aggressively.This algorithm does not include voided urine cytology because of its low sensitivity. However,since the specificity of urine cytology is very high, further evaluation including ureteroscopy may not be needed in patients with tumor-like lesions detected by CT and positive voided urine cytology[13].Further study with a large population will be needed to confirm this algorithm.
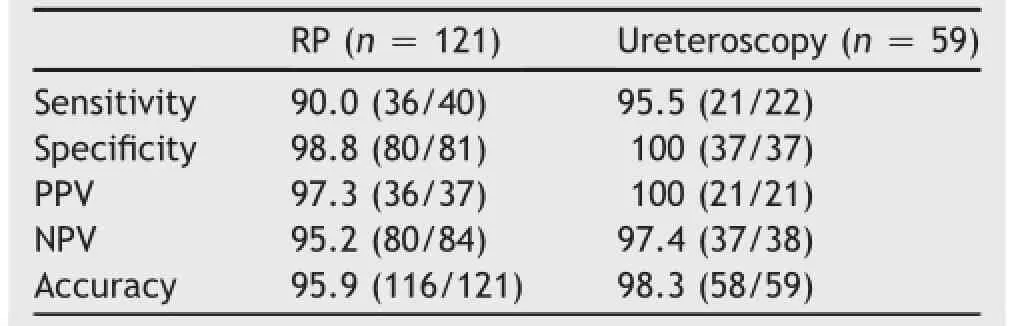
Table 3Diagnostic accuracy of RP and ureteroscopy for UUTUC in all 125 patients(%).
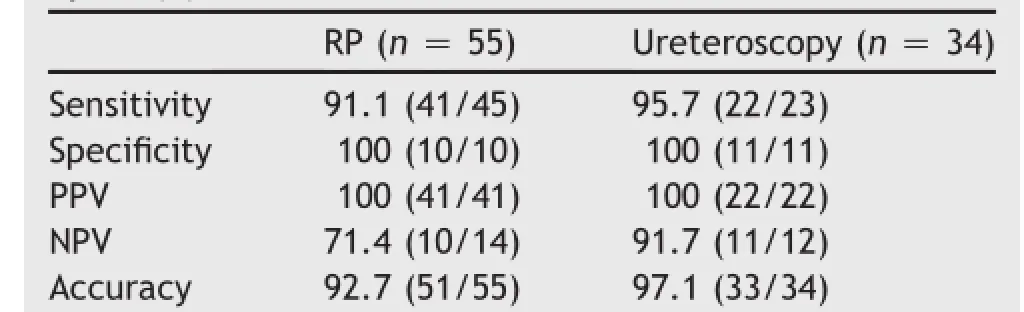
Table 4Diagnostic accuracy of RP and ureteroscopy for UUTUC in 58 patients who had tumor-like lesions revealed by CT(%).
Our study had several limitations.First,this study is retrospective.Second,we only included the patients who underwent examination of the UUT.Therefore patients who were judged to have UUTUCs only by CT findings but who did not undergo further examination of the UUT were not included in this study.Third,not all patients underwent RP and ureteroscopy because the method of evaluation was decided by the physician-in-chief.Therefore there is a possibility of patient selection bias.Some included patients received only semi-rigid ureteroscopy and not flexible ureteroscopy because they were seen before the introduction of flexible ureteroscopy.The diagnostic accuracy of ureteroscopy for tumors in the renal pelvis is likely to have improved after the introduction of flexible ureteroscopy compared with that of only semi-rigid ureteroscopy.Thus the diagnostic accuracy is recently estimated to be higher.
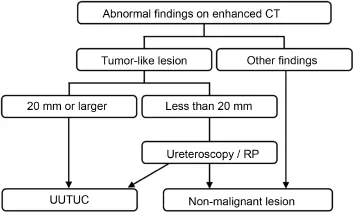
Figure 3The strategy to evaluate the UUT to detect UUTUC. UUT,upper urinary tract;CT,computed tomography;RP, retrograde pyelography;UUTUC,upper urinary tract urothelial cancer.
5.Conclusion
Enhanced CT is a suitable method for examining the UUT. We can decide to evaluate the possibility of UUTUCs according to the tumor diameter on CT.When we do so ureteroscopy is recommended.
Conflicts of interest
The authors declare no conflict of interest.
[1]Kitamura H,Maeda T,Tanaka T,Fukuta F,Kobayashi K, Nishiyama N,et al.Comparison of laparoscopic,hand-assisted, and open surgical nephroureterectomy.JSLS 2014;18:288-93.
[2]Lisanti CJ,Toffoli TJ,Stringer MT,DeWitt RM,Schwope RB.CT evaluation of the upper urinary tract in adults younger than 50 years with asymptomatic microscopic hematuria:is IV contrast enhancement needed?AJR Am J Roentgenol 2014; 203:615-9.
[3]Shao P,Li P,Xu Y,Cao Q,Ju X,Qin C,et al.Application of combined computed tomography arteriography,venography, and urography in laparoscopic partial nephrectomy with segmental artery clamping.Urology 2014;84:1361-5.
[4]LiC,Lin X,HuiC,Lam KM,Zhang S.Computer-aided diagnosis for distinguishing pancreatic mucinouscystic neoplasms fromserous oligocystic adenomas in spectral CT images.Technol Cancer Res Treat 2014.pii:1533034614563013.[Epub ahead of print].
[5]Ohkawa K,Imanaka K,Sakakibara M,Tamai C,Ishihara A, Hasegawa N,et al.Factors related to shift from hepatic borderline lesion to overt HCC diagnosed by CT.Hepatogastroenterology 2014;61:1680-7.
[6]Matsuki M,Takahashi A,Katou S,Takayanagi A,Takagi Y, Kamata K.Pathological complete response to gemcitabine and cisplatin chemotherapy for advanced upper tract urothelial carcinoma:a case report.Nihon Hinyokika Gakkai Zasshi 2013; 104:33-7[in Japanese].
[7]Fulgham PF,Bishoff JT.Urinary tract imaging:basic principles.In:Wein AJ,Kavoussi LR,Campbell MF,editors.Campbell-Walsh urology.10th ed.,vol.1.Philadelphia:Saunders, an imprint of Elsevier Inc;2012.p.107-8.
[8]Duffey B,Monga M.Upper urinary tract endoscopy.In: Wein AJ,Kavoussi LR,Campbell MF,editors.Campbell-Walsh urology.10th ed.,vol.1.Philadelphia:Saunders,an imprint of Elsevier Inc;2012.p.196-203.
[9]Kanda Y.Investigation of the freely available easy-to-use software‘EZR’for medical statistics.Bone Marrow Transplant 2012;48:452-8.
[10]Akobeng AK.Understanding diagnostic tests 3:receiver operating characteristic curves.Acta Paediatr 2007;96:644-7.
[11]Caoili EM,Cohan RH,Inampudi P,Ellis JH,Shah RB, Faerber GJ,et al.MDCT urography of upper tract urothelial neoplasms.AJR Am J Roentgenol 2005;184:1873-81.
[12]Maheshwari E,O’Malley ME,Ghai S,Staunton M,Massey C. Split-bolus MDCT urography:upper tract opacification and performance for upper tract tumors in patients with hematuria.AJR Am J Roentgenol 2010;194:453-8.
[13]Takao A,Saika T,Uehara S,Monden K,Abarzua F,Nasu Y, et al.Indications for ureteropyeloscopy based on radiographicfindings and urine cytology in detection of upper urinary tract carcinoma.Jpn J Clin Oncol 2010;40:1087-91.
Received 26 July 2015;received in revised form 9 September 2015;accepted 5 November 2015
Available online 26 November 2015
*Corresponding author.
E-mail address:aktakaya@sapmed.ac.jp(A.Takayanagi).
Peer review under responsibility of Shanghai Medical Association and SMMU.
http://dx.doi.org/10.1016/j.ajur.2015.11.005
2214-3882/?2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
 Asian Journal of Urology2016年1期
Asian Journal of Urology2016年1期
- Asian Journal of Urology的其它文章
- Unusual case of nephrocutaneous fistula-Our experience
- A case of giant prostatic hyperplasia
- Tumour lysis syndrome:A rare acute presentation of locally advanced testicular cancer-Case report and review of literature
- Can intravesical prostatic protrusion predict bladder outlet obstruction even in men with good flow?
- Zoledronic acid combined with androgendeprivation therapy may prolong time to castration-resistant prostate cancer in hormone-na?ve metastatic prostate cancer patients-A propensity scoring approach
- Prostate cancer volume associates with preoperative plasma levels of testosterone that independently predicts high grade tumours which show low densities(quotient testosterone/tumour volume)