Efficacy and safety of the Chinese herbal medicine shuganjieyu with and without adjunctive repetitive transcranial magnetic stimulation (rTMS) for geriatric depression: a randomized controlled trial
2015-12-09 05:19:36MinminXIEWenhaiJIANGHaiboYANG
上海精神醫學 2015年2期
Minmin XIE, Wenhai JIANG,2*, Haibo YANG,2
Efficacy and safety of the Chinese herbal medicine shuganjieyu with and without adjunctive repetitive transcranial magnetic stimulation (rTMS) for geriatric depression: a randomized controlled trial
Minmin XIE1, Wenhai JIANG1,2*, Haibo YANG1,2
shuganjieyu; Chinese herbal medicine; repetitive transcranial magnetic stimulation; geriatric depression; China
1. Background
Depression is a common mental disorder and a leading cause of disease burden in the elderly population.According to data from the World Health Organization,the prevalence of depression in elderly individuals is between 3 and 10%.[1]Geriatric depression usually refers to depression among individuals 60 years of age or older.[2]Slow onset and atypical symptoms (e.g.,relatively mild depressive symptoms and frequent concurrent somatic symptoms) are common in geriatric depression, which makes it easy to overlook. Failure to identify and treat geriatric depression can exacerbate the decline in physical functioning due to concurrent physical illnesses, increase the level of disability, and,thus, substantially decrease the individual’s quality of life.[3]
Using a selective serotonin re-uptake inhibitor (SSRI)is the recommended first-line treatment for geriatric depression in most high-income countries. But these medications have many side-effects – some of which are serious[4]– that increase in prevalence and severity with increased dosage and that may be more prevalent and less tolerated in elderly individuals. The initial dose of antidepressant medication used for geriatric depression is usually relatively low due to clinicians’ concerns about serious side effects or interactions with other medications being used for physical illnesses. Partly due to this reason (i.e., using sub-optimal dosages),the treatment effect of common antidepressants in geriatric depression is not as robust as that in younger adults; moreover, geriatric patients who consider the medications less effective are often non-compliant with anti-depressant treatment. Many of these untreated or inadequately treated individuals become chronically depressed.
Chinese herbal medicines have been widely used in the treatment of depression. Shuganjieyu, which is composed of St. John’s wort and extracts of Siberian ginseng, is the first Chinese herb-based medication approved by the Chinese drug regulatory agency(CFDA) for the treatment of depression (approved in 2008). It has been shown to be effective, safe, and well tolerated.[5-7]The main ingredients of shuganjieyu are hypericum perforatum and acanthopanax extract. The antidepressant effect of hypericum perforatum, which has a mechanism of action similar to that of SSRIs, has been well recognized.[8]Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive intervention that has also been shown to be a safe and effective treatment for depression in China and abroad.[9-11]This study aims to evaluate the efficacy and safety of shuganjieyu for geriatric depression when used with or without adjunctive treatment with rTMS.
2. Methods
2.1 Sample
Figure 1 shows the enrollment of subjects in the study.Study participants were 79 patients with geriatricdepression admitted to the Third Hospital of Daqing Municipality between December 2013 and September 2014. The inclusion criteria were as follows. (a) Met the diagnostic criteria for depression according to the 10thedition of the International Classification of Diseases(ICD-10)[12]and had not been taking antidepressants in the two weeks prior to enrollment. (b) Met the classification of ‘liver stagnation and spleen deficiency’based on Traditional Chinese Medicine theories.[13][Symptoms of stagnated liver energy (‘qi’) include uncoordinated mood and will, lack of aspiration, and low mood; symptoms of spleen deficiency include emotional distress, restlessness, poor memory,insomnia, dizziness and poor appetite.] (c) Aged 60 years or older. (d) Scored no less than 18 points on the 17-item version of the Hamilton Rating Scale for Depression (HAMD-17).[14](e) Were willing to participate and signed the informed consent form (or their guardian signed the consent form). (f) Were in good physical health based on the baseline physical examination,electrocardiogram (EKG), clinical laboratory test results,and medical history. Exclusion criteria included (a)having suicidal tendencies; (b) the presence of serious heart, liver, or kidney dysfunction or any disease of the endocrine system; (c) had a history of epilepsy; (d)had a history of psychoactive substance dependence(including alcohol); (e) had depression induced by other mental or physical conditions; (f) had a bipolar disorder; (g) were unfit for rTMS treatment; (h) were allergic to hypericum perforatum or acanthopanax; (i)had abnormal EKG or laboratory test results; (j) had a history of poor medication compliance; or (k) had received electroconvulsive therapy in the month prior to enrollment.

Figure 1. Flowchart of the study
2.2 Intervention
Patients who met the inclusion criteria were randomly assigned to the experiment or control group using a random number table. Shuganjieyu provided by Chengdu Kanghong Pharmaceuticals Co. Ltd., (China SFDA No. Z20080580) were used in the study. Patients in both groups received two capsules of shuganjieyu immediately after meals, twice a day for six weeks.Participants in the experiment group were also treated with rTMS (using equipment from the Magstim Co.,Ltd, UK) with the coil located above the left dorsolateral prefrontal cortex; participants in the control group were given mock-rTMS in which the coil touched the scalp but no stimulation was provided. The rTMS stimulation was of low intensity (30% MT) and low frequency (10HZ).Each session lasted for an average of 20 minutes. A total of 20 rTMS sessions were administered in four 5-day cycles with 2-day breaks between cycles. All participants and evaluators were masked during the trial. For patients who experienced sleep problems during the treatment, zopiclone or benzodiazepines were allowed for short-term treatment.
2.3 Assessment of efficacy
The Hamilton Rating Scale for Depression-17 Item(HAMD-17) was used to assess efficacy and the Treatment Emergent Symptom Scale (TESS) was used to assess safety.[14]The two scales were administered at 1 week, 2 weeks, 4 weeks, and 6 weeks after the initiation of the treatment. The reported inter-rater reliability of the Chinese version of HAMD-17, based on the correlation of total scores between independent raters, is between 0.88 and 0.99 and its validity, based on the correlation or the total score and clinical ratings of the severity of depression, is 0.92.[15]Two trained associate senior clinicians conducted these evaluations in this study; the inter-relater reliability of their HAMD-17 total was good (Kappa 0.75 to 0.86). Routine blood tests, tests of liver and kidney function, and EKGs were also assessed at the same time periods.
The main measure of efficacy was the percent reduction from baseline HAMD-17 scores ([pretreatment score - post-treatment score]/pretreatment score x 100%) at the end of the trial. Efficacy was categorized into remitted (reduction >75% or total HAMD-17 score <7), significantly improved(reduction=50 to 74%), improved (reduction=25 to 49%), and not improved (reduction <25%).
The HAMD-17 can be divided into 5 subscales:[16,17](a) 4 items in the retardation subscale assess depressed mood, work and activities, psychomotor retardation,and loss of sexual interest; (b) 3 items assess guilt,suicidal ideation, and psychomotor agitation; (c) 3 items assess sleep problems including difficulty of falling asleep, light sleep, and early awakening; (d) 6 items assess anxiety and somatic symptoms including mental anxiety, somatic anxiety, gastrointestinal symptoms,hypochondriasis, insight, and general somatic symptoms. And (e) 1 item assesses loss of weight.
2.4 Statistical analysis
SPSS 19.0 was used for data analysis. Means and standard deviations were provided. ANCOVA and repeated measures ANOVA (for HAMD-17 scores) were used to compare differences over time and cross groups.Two-sample t-test was used to compare cross-group differences and one-sample t-test was used to assess within-group differences (i.e., compared to baseline).Chi-squared test was used to compare categorical variables and Mann-Whitney rank test was use to compare continuous variables that were not normally distributed.
3. Results
3.1 Characteristics of participants
Figure 1 shows the flowchart for the study. A total of 65 patients met the inclusion criteria, among whom 36 were assigned to the experiment group and 29 to the control group. In the experiment group, 1 patient dropped out from the study due to early hospital discharge; in the control group the diagnosis was changed to schizophrenia 1 week after admission in 1 patient and another 2 patients dropped out of the study because of early hospital discharge. Therefore, the final analysis included 35 individuals in the experiment group and 26 in the control group. The study completion rate was 97.2% (35/36) in the experimental group and 89.7% (26/29) in the control group. Table 1 shows the characteristics of the individuals who completed the 6-week study; there are no significant differences in gender, age, duration or illness or baseline total HAMD-17 total score between the two groups.
3.2 Comparison of efficacy
As shown in Table 2, based on the results of the repeated measures ANOVA, there were no significant cross-group differences (F=0.46,p=0.502) or differences in group-time interaction (F=1.07,p=0.352) in HAMD-17 total scores. However, HAMD-17 scores changed significantly over time (F=395.91,p<0.001). There was a gradual decrease in the measured severity of depressive symptoms over the six weeks of treatment that was similar in the two groups; by the end of the 6 weeks the mean HAMD-17 score in both groups had dropped by more than 37%.
At the end of the trial (after 6 weeks of treatment),the two groups had similar efficacy. Using the classification system described in the methods section based on the percent change in the baseline HAMD-17 score, among the 35 patients in the experimental group who completed the 6 weeks of treatment, 1 had fully remitted, 6 were significantly improved, 27 were improved, and 1 was unchanged; thus the overall efficacy was 97.1% (34/35). Among the 26 patients in the control group who completed the treatment,1 had fully remitted, 4 were significantly improved,20 were improved, and 1 was unchanged; thus the overall efficacy was 96.2% (25/26). However, among the 61 patients from both groups who completed 6 weeks of treatment, only 2 (3.3%) remitted and only a further 10 (16.4%) had significant improvement; the remaining 80.3% (49/61) had less than 50% reduction in their baseline HAMD-17 scores. That is, by the end of the trial only 20% (7/35) of experimental groups subjects and 19% (5/26) of control groups subjects had experienced significant improvement (or remission) of their depressive symptoms.
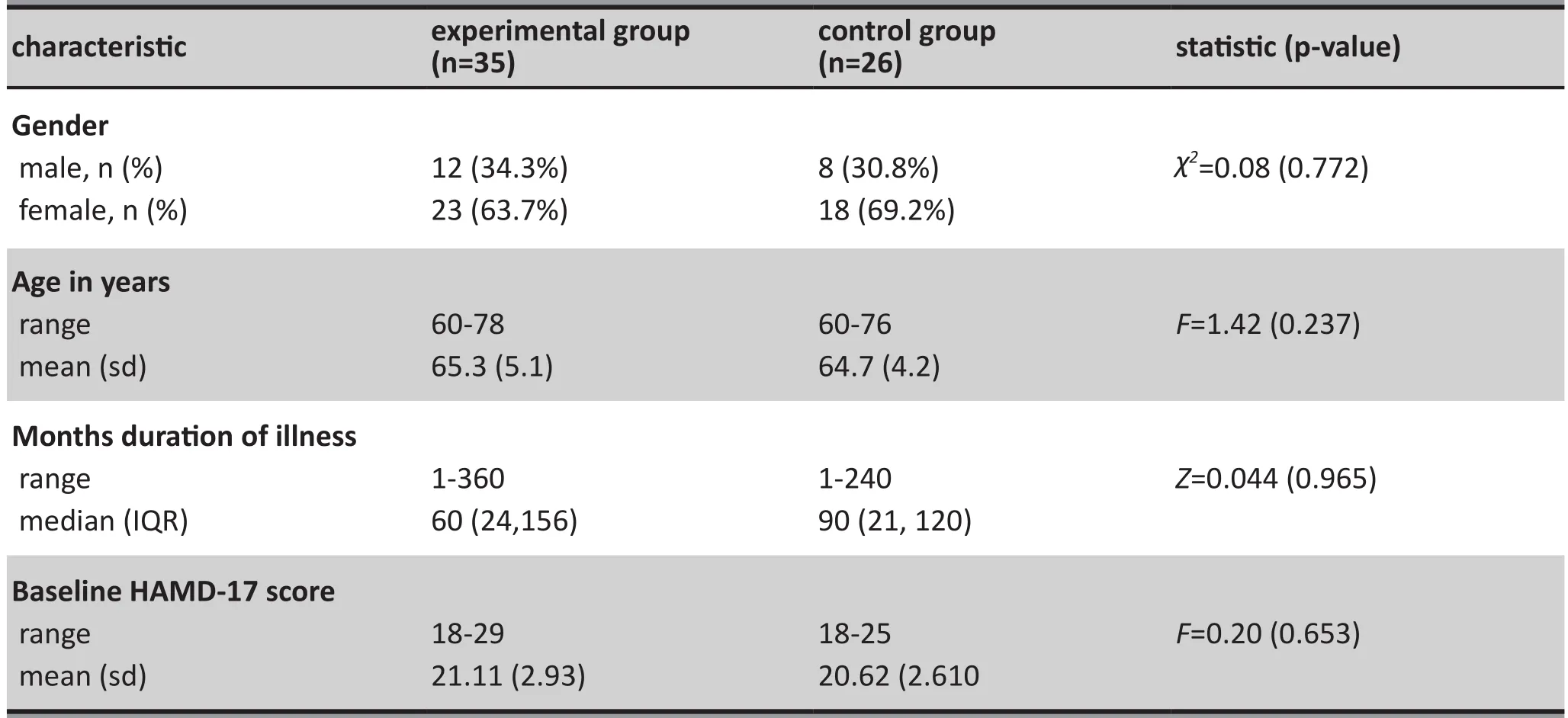
Table 1. Characteristics of study participants
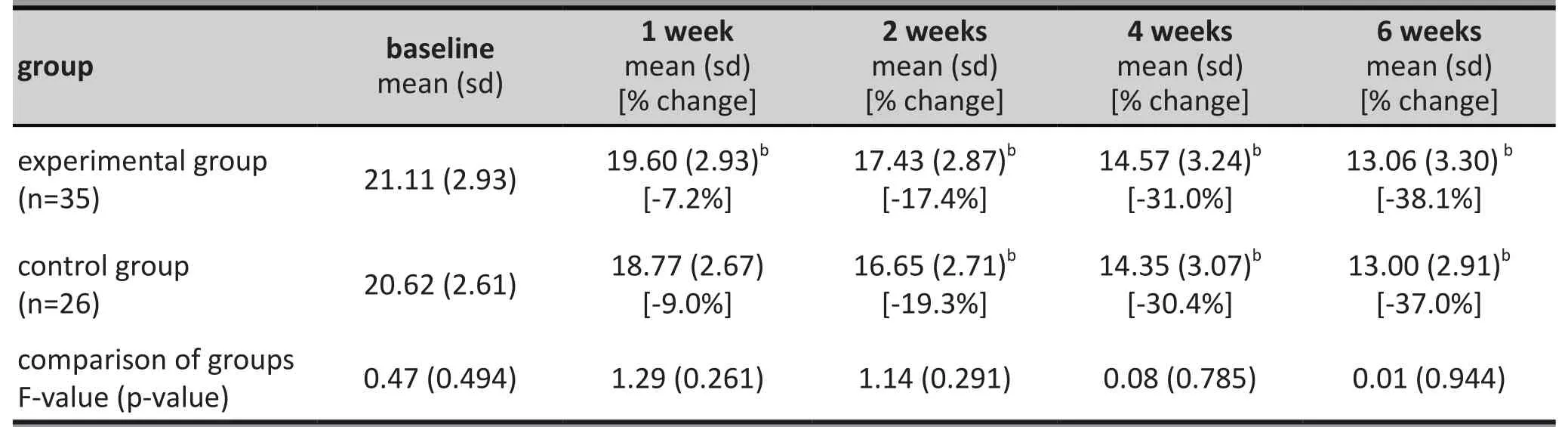
Table 2. Comparison of mean (sd) Hamilton Depression Rating Scale (HAMD-17) scores andthe percent change in the scores from baseline during the 6 weeks of treatment in theexperimental and control groupsa
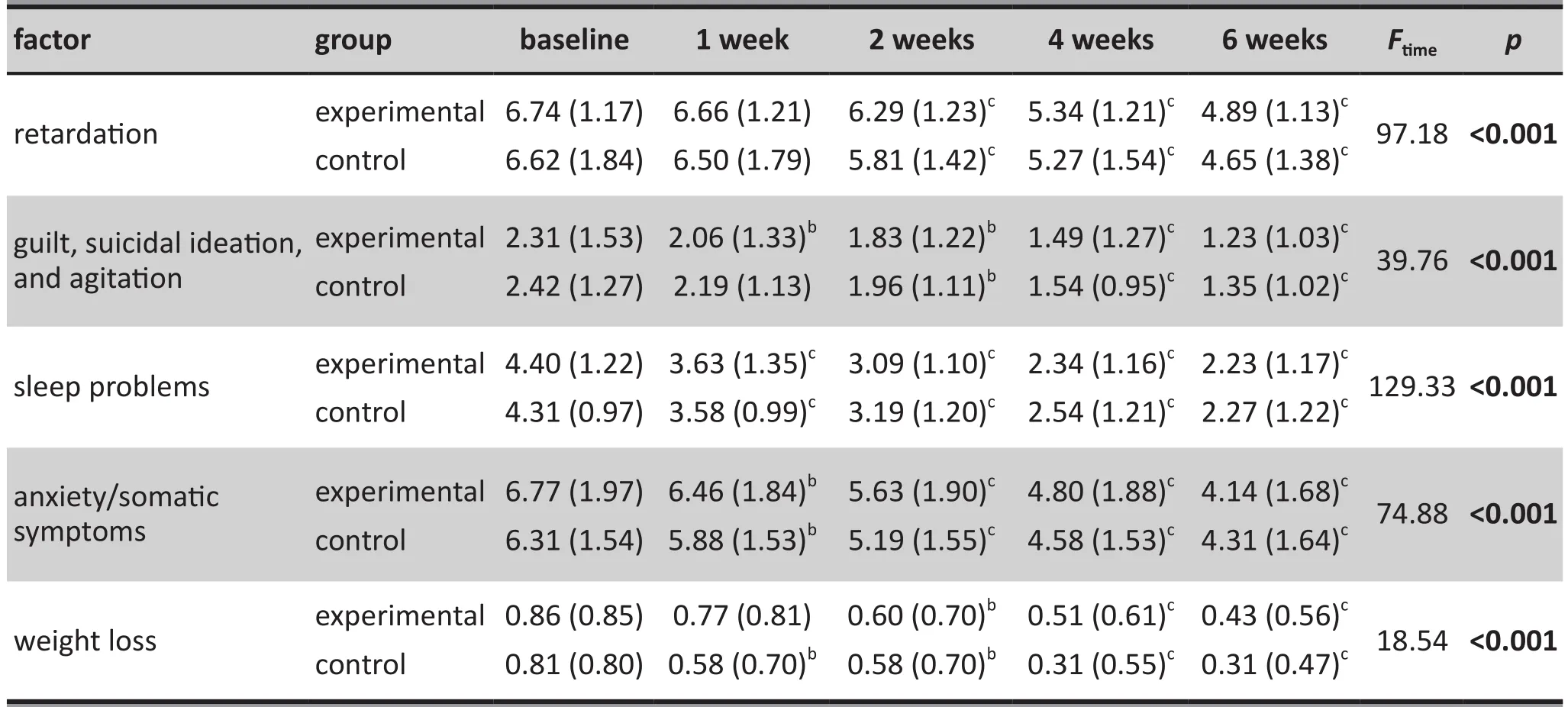
Table 3. Comparison of mean (sd) factors scores of Hamilton Depression Rating Scale (HAMD-17)before and after treatment in the experimental and control groupsa
Table 3 presents comparisons of the five HAMD-17 subscale scores. All of the subscales showed a dramatic drop in the mean scores over the 6 weeks of the trial,but there were no significant differences between the experimental and control groups in the magnitude or pace of the improvement. There were some minor differences in the rate of improvement for the five subscales: after 1 week of treatment, the improvement in sleep and anxiety/somatic symptoms had already become statistically significant, the improvement in weight loss was only significant in the control group,the improvement in the ‘guilt, suicidal ideation,and agitation’ subscale was only significant in the experimental group, and neither of the groups showed statistically significant improvement in psychomotor retardation. However, by the end of the second week of treatment both groups showed statistically significant improvement over baseline in all five HAMD-17 subscales scores.
3.3 Comparison of safety
No severe adverse events occurred during the trial.Most adverse events occurred early in the study.There were a total of 15 events in 14 individuals (40%)in the experiment group: 2 had dry mouth (5.7%), 3 had headaches or discomfort in the head (8.6%), 2 experienced dizziness (5.7%), 3 had constipation (8.6%),3 had nausea (8.6%), 1 had excessive sweating (2.9%),and 1 had poor appetite (2.9%). There were a total of 13 events in 13 individuals (50%) in the control group:3 had dry mouth (11.5%), 2 had headaches (7.7%),4 experienced dizziness (15.4%), 1 had a stuffy nose(3.85%), 1 had constipation (3.9%), 1 had diarrhea(3.9%), and 1 had poor appetite (3.9%). All of these adverse events remitted spontaneously without any treatment; none of them were severe enough to require discontinuation of the treatment. The proportions of patients in the experimental and control groups who experienced adverse events were not statistically significant (40% v. 50%;χ2=0.605,p=0.437).
4. Discussion
4.1 Main findings
In this double-blind randomized controlled trial that used changes in HAMD-17 total scores as the main outcome measure, we found comparable effectiveness of the Chinese herbal medicine shuganjieyu with or without adjunctive rTMS in the inpatient treatment of geriatric depression. Ninety-four percent (65/69) of the enrolled subjects completed the 6-week trial. None of the patients experienced serious side effects. Minor side effects occurred in 40% of patients treated with shuganjie and rTMS (the experimental group) and in 50% of patients treated with shuganjie and sham rTMS(the control group); all of these side effects resolved spontaneously and none of them required withdrawal from the study. We conclude that combined treatment with shuganjieyu and rTMS is safe.
Improvement in depressive symptoms was progressive over the 6-week trial; by the end of the 6 weeks the mean overall HAMD-17 score had dropped by 38% in the experimental group and 37% in the control group. The failure to identify a significant time by group interaction in the repeated measures ANOVA suggests that rTMS does not result in a more rapid onset of treatment, as has been suggested by other authors.[11]Using a drop in HAMD-17 score from baseline of 25%or greater as the cutoff for ‘efficacy’, by the end of the trial efficacy was 97% in the experimental group and 96% in the control group. However, using a drop in the HAMD-17 score from baseline of 50% or greater as the cutoff for ‘significant improvement’, only 20% (7/35) of the patients in the experimental group and 19% (5/26)of the patients in the control group had a significant improvement in their depressive symptoms by the end of the 6 weeks of treatment.
When considering the five subscales of HAMD-17,there were some minor, non-significant differences in the onset of the treatment effect between the different subscales, but all five subscales showed statistically significant improvement after two weeks of treatment in both treatment groups.
4.2 Limitations
The 97% ‘efficacy’ of shuganjieyu appears promising but the picture looks quite different when one realizes that only 20% of patients had a 50% or greater improvement in their depressive symptoms over the 6-week trial.In the absence of a full placebo control group or an SSRI comparison group one cannot be certain that the observed improvement in both groups was the result of shuganjieyu treatment -- it could have been related to the placebo effect of being hospitalized. Studies using different types of comparison groups will be needed to resolve this issue.
This study was conducted in an inpatient setting with patients who had relatively severe depressive symptoms. It is unknown whether or not the outcome would be the same in less-severe, community-based patients. In particular, the use of rTMS, which required daily sessions at a medical setting over several weeks,may not be feasible for most community-based patients.
The failure to find any significant differences between the two groups may be because we did not use the optimal configuration, frequency, and duration of rTMS. The optimal parameters may be different in elderly individuals, so considerable work will be needed to establish standardized methods for administering rTMS in geriatric depression. Larger studies conducted for longer periods may identify significant differences when rTMS is used as an adjunctive treatment for shuganjieyu, but this would probably only be practical in inpatient settings. There may be specific subgroups of patients for whom rTMS is a useful adjunctive treatment, but larger studies would be needed to compare differences between different subgroups of patients to help identify the subgroups in which rTMS is useful.
4.3 Implications
We confirm the efficacy and safety of the Chinese herbal medicine shuganjieyu in the treatment of geriatric depression. However, after 6 weeks of treatment only 20% of the subjects had a significant improvement in their depressive symptoms (defined as a 50% drop in the baseline HAMD-17 score) so the value of this medicine as a first-line treatment for geriatric depression may be limited. Shuganjieyu may, however, be useful as a second-line treatment for elderly individuals who cannot tolerate SSRIs. We did not find that adjunctive treatment with rTMS improved overall outcomes for shuganjieuyu or resulted in a more rapid onset of action,though larger samples and longer follow-up studies may be needed to definitively address this issue.
Conflict of interest
The authors declare no conflict of interest.
Funding
The authors obtained no funding to support this study.
Ethics approval
This study was approved by the ethics committee of Daqing Third Hospital.
Informed consent
All participants or their guardians provided informed consent to participate in this study.
1. Lingworth SA, Burgess PM, Whiteford HA. Affective and anxiety disorders: prevalence, treatment and antidepressant medication use.Aust N Z J Psychiatry. 2010; 44(6): 513-519
2. Clignet F, van Meijel B, vail Straten A, Cuijpers P. The systematic activation method as a nursing intervention in depressed elderly: a protocol for a multi-centre cluster randomized trial.BMC Psychiatry.2012; 12(1): 144. doi:http://dx.doi.org/10.1186/1471-244X-12-144
3. Li J. [Efficacy observation of the sertraline treatment combined with Shuganjieyu capsule on the elderly patients with depression].Zhongguo Yi Yao Zhi Nan. 2013; 11(34):495-496. Chinese
4. Digby G, Machaalany J, Malik P, Methot M, Simpson CS, Redfearn D, et al. Multifactorial QT interval prolongation.Cardiol J. 2010; 17(2): 184-188
5. Liu SB, Li CF, Wang YF, Li J. [Case-control study of the treatment of Shuganjieyu capsule combined with venlafaxine on the elderly patients with depression].Lin Chuang Jing Shen Yi Xue Za Zhi. 2012; 22(2): 98. Chinese
6. Song H, Ma JD, Chen YX, Huang SP. [The efficacy of Shuganjieyu capsule combined with venlafaxine in treatment of senile depression].Yi Xue Zong Shu. 2013;19(17): 2302-2308. Chinese. doi: http://dx.doi.org/10.3969/j.issn.1006-2084.2013.17.043
7. Alexopoulos GS, Kelly RE. Research advances in geriatric depression.World Psychiatry. 2009; 8(3): 140-149
8. Russo E, Scicchitano F, Whalley BJ, Mazzitello C, Ciriaco M, Esposito S, et al. Hypericumperforatum: pharmacokinetic,mechanism of action, tolerability, and clinical drug-drug interactions.Phytother Res. 2014; 28(5): 643-655. doi:http://dx.doi.org/10.1002/ptr.5050
9. Dumas R, Padovani R, Richierij R, Lan?on C. [Repetitive transcranial magnetic stimulation in major depression:response factor].Encephale. 2012; 38(4): 360-368. French.doi: http://dx.doi.org/10.1016/j.encep.2011.08.004
10. Richieri R, Guedj E, Michel P, Lan?on C, Boyer L. Maintenance transcranial magnetic stimulation reduces depression relapse: a propensity-adjusted analysis.J Affect Disord.2013; 151(1): 129-135. doi: http://dx.doi.org/10.1016/j.jad.2013.05.062
11. Schutter DJ. Quantitative review of the efficacy of slowfrequency magnetic brain stimulation in major depressive disorder.Psychol Med. 2010; 40(11): 1789-1795
12. World Health Organization.ICD-10 Classifications of Mental and Behavioural Disorder: Clinical Descriptions and Diagnostic Guidelines.Geneva: World Health Organization;1992
13. Dong HT, Han G, Zhu XC, Guo RJ. [Progress on depression due to liver stagnation and spleen deficiency: a literature review].Huan Qiu Zhong Yi Yao. 2014; 7(2): 46-50. Chinese. doi:http://dx.doi.org/10.3969/j.issn.1674-1749.2014.02.022
14. Zhang MY. [Manual of Psychiatric Rating Scale]. Changsha:Hunan Science and Technology Press; 1998. p. 121-204.Chinese
15. Dan B. [Assessment on diagnosis and efficacy of Han Mitton Depression Scale for 136 cases of post-stroke depression].Zhongguo Wu Zhen Xue Za Zhi. 2007; 7(24):5848-5849. Chinese. doi: http://dx.doi.org/10.3969/j.issn.1009-6647.2007.24.129
16. Chen YY, Wang YJ, Huang Y. [The effects on the score of the each factor of HAMD for mild to moderate depression treated with abdominal acupuncture].Liao Ning Zhong Yi Za Zhi. 2011; 38(5): 981-983. Chinese
17. Chen JD. [Clinical and neuroimaging studies of depression in elderly]. Hu Nan, Changsha: Central South University; 2008.Chinese
, 2015-03-18; accepted, 2014-04-09)

Minmin Xie obtained her bachelor’s degree in medicine from Harbin Medical University (Daqing Campus) in June 2013. She enrolled in a master’s program at Harbin Medical University (Daqing Campus) in 2013 and is currently doing her internship at the Geriatrics Department of the Third Hospital of Daqing. Her research interest is the treatment of geriatric mental disorders.
中草藥舒肝解郁膠囊單用或聯合重復經顱磁刺激(rTMS)治療老年期抑郁癥的療效和安全性:一項隨機對照研究
謝敏敏,姜文海,楊海波
舒肝解郁膠囊;中草藥;重復經顱磁刺激;老年期抑郁癥;中國
Background: Pharmacological treatment of geriatric depression is often ineffective because patients cannot tolerate adequate doses of antidepressant medications.Aims: Examine the efficacy and safety of shuganjieyu – the first Chinese herbal medicine approved for the treatment of depression by China’s drug regulatory agency -- with and without adjunctive treatment with repetitive transcranial magnetic stimulation (rTMS) in the treatment of geriatric depression.Methods: Sixty-five inpatients 60 or older who met ICD-10 criteria for depression were randomly assigned to an experimental group (shuganjieyu + rTMS) (n=36) or a control group (shuganjieyu + sham rTMS)(n=29). All participants
4 capsules of shuganjieyu daily for 6 weeks. rTMS (or sham rTMS)was administered 20 minutes daily, five days a week for 4 weeks. Blinded raters used the Hamilton Rating Scale for Depression (HAMD-17) and the Treatment Emergent Symptom Scale to assess clinical efficacy and safety at baseline and 1, 2, 4, and 6 weeks after starting treatment. Over the six-week trial, there was only one dropout from the experimental group and two dropouts from the control group.Results: None of the patients had serious side effects, but 40% in the experimental group and 50% in the control group experienced minor side effects that all resolved spontaneously. Both groups showed substantial stepwise improvement in depressive symptoms over the 6 weeks. Repeated measures ANOVA found no differences between the two groups. After 6 weeks, 97% of the experimental group had experienced a 25% or greater drop in the level of depression, but only 20% had experience a 50% or greater drop in the level of depression; the corresponding values in the control group were 96% and 19%.There were some minor, non-significant differences in the onset of the treatment effect between the different types of depressive symptoms, but by the second week of treatment all five HAMD-17 subscale scores had improved signi ficantly in both groups Conclusions: The Chinese herbal medicine shuganjieyu is effective and safe in the treatment of geriatric depression, but only a minority of patients have greater than 50% improvement in their depressive symptoms after 6 weeks of treatment. Adjunctive use of rTMS with shuganjieyu does not improve the overall outcome and does not signi ficantly speed up the onset of action of shuganjieyu.
[Shanghai Arch Psychiatry. 2015; 27(2): 103-110.
http://dx.doi.org/10.11919/j.issn.1002-0829.214151]
1Daqing Campus of Harbin Medical University, Daqing, Heilongjiang Province, China
2The Third People’s Hospital of Daqing, Daqing, Heilongjiang Province, China
*correspondence: dqjwh@126.com
背景:由于老年期抑郁癥患者往往不能耐受足量的抗抑郁藥物,所以藥物治療老年抑郁癥的療效不佳。目的:探討舒肝解郁膠囊(中國藥品監督管理部門批準用于治療抑郁癥的首個中草藥)單用或聯合重復經顱磁刺 激(repetitive transcranial magnetic stimula-tion,rTMS)治療老年期抑郁癥的療效和安全性。方法:將65例60歲以上符合ICD-10診斷標準的抑郁癥住院患者隨機分為研究組(舒肝解郁膠囊+rTMS)(n =36)和對照組(舒肝解郁膠囊+偽rTMS)(n=29)。所有患者每日服用4粒舒肝解郁膠囊,一共服用6周。rTMS(或偽rTMS)治療20 min/d,每周5 d,共4周。評估者在不知患者分組情況下,采用漢密爾頓抑郁量表(HAMD-17)和副反應量表評估基線和治療開始后1、2、4、6周的臨床療效和安全性。在6周的研究過程中,研究組僅有1人脫落,對照組僅有2人脫落。結果:沒有一例患者出現嚴重不良反應,但研究組和對照組中分別有40%和50%的患者出現輕微的不良反應,均自行緩解。兩組的抑郁癥狀在6周內均逐步明顯改善。重復測量方差分析沒有發現兩組之間有顯著差異。 6周后,研究組97%的患者抑郁程度下降幅度大于等于25%,但只有20%者的下降幅度大于等于50%;對照組中相應的患者比例分別為96%和19%。雖然不同的抑郁癥狀之間治療起效有著輕微的、非顯著性的差異,但是治療第二周后兩組HAMD-17五個分量表的評分均顯著改善。結論:中草藥舒肝解郁膠囊治療老年抑郁癥是有效和安全的,然而只有少數患者的抑郁癥狀在治療6周后改善程度大于50%。聯合重復經顱磁刺激治療并沒有增加舒肝解郁膠囊的總體療效,也沒有顯著加快后者的起效。
本文全文中文版從2015年6月6日起在http://dx.doi.org/10.11919/j.issn.1002-0829.214151 可供免費閱覽下載
猜你喜歡
現代儀器與醫療(2022年2期)2022-08-11 09:51:40
汽車工程師(2021年12期)2022-01-18 06:02:43
今日農業(2021年17期)2021-11-26 23:38:44
今日農業(2020年18期)2020-12-14 19:08:44
中華養生保健(2020年1期)2020-11-16 00:47:38
中國中醫急癥(2019年10期)2019-05-21 07:20:30
中國醫藥指南(2017年3期)2017-11-13 02:57:31
廣東飼料(2016年7期)2016-12-01 03:43:34
信息安全與通信保密(2016年3期)2016-08-23 01:23:46
林業與生態(2016年3期)2016-02-27 14:24:13
- 上海精神醫學的其它文章
- Decision tree methods: applications for classi fication and prediction
- Case report of visual hallucinations in anxiety
- Clinical and research value of the new diagnostic criteria for Alzheimer’s disease
- Are the revised diagnostic criteria for Alzheimer’s disease useful in low- and middle-income countries?
- Gene-based and pathway-based genome-wide association study of alcohol dependence
- Prenatal choline and the development of schizophrenia