急性血液稀釋技術在動物實驗圍手術期中的應用
2015-05-11 11:13:49朱澤興張樹明趙永軍樊凱彬
中國比較醫學雜志 2015年4期
朱澤興,張樹明,趙永軍,樊凱彬,喬 林
(1.解放軍第二炮兵總醫院骨科,北京 100088;2.武警醫學院附屬醫院骨科,天津 300160;3.邯鄲市中心醫院骨科,邯鄲河北 056001)
急性血液稀釋技術在動物實驗圍手術期中的應用
朱澤興1,張樹明1,趙永軍2,樊凱彬3,喬 林1
(1.解放軍第二炮兵總醫院骨科,北京 100088;2.武警醫學院附屬醫院骨科,天津 300160;3.邯鄲市中心醫院骨科,邯鄲河北 056001)
目的觀察急性血液稀釋技術(ANH)在狗斷肢冷凍再植實驗中對改善術中、術后動物全身狀態的作用。方法 在狗后肢深低溫冷凍再植實驗中,對照組(A組)采用靜脈補充等量乳酸鈉林格氏液,實驗組(B組)采用急性血液稀釋技術,對比兩組各時點循環動力學指標、血常規、術后動物蘇醒時間、抬頭時間、站立時間、術后進食、進水時間。結果 ①術中兩組PaO2、PCO2值均在正常范圍,呼吸頻率正常,B組心率明顯低于A組,術中血紅蛋白、紅細胞壓積輸血前A組與B組無統計學差異,術后B組明顯高于A組,差異存在顯著性。②術后動物蘇醒時間、抬頭時間、站立時間、術后進食量、進水量B組均明顯優于A組,存在顯著差異。結論 在狗斷肢深低溫冷凍再植實驗中,急性血液稀釋技術(ANH)能明顯改善動物術中的全身狀態,加快術后恢復速度。
自體輸血;急性血液稀釋技術(ANH);斷肢再植;冷凍保存;外科手術
復雜手術動物實驗往往手術時間長、創傷大、出血多,容易造成術中、術后動物休克死亡而使實驗失敗。由于目前尚無實驗動物異體血庫,無法進行異體輸血,所以我們在狗后肢深低溫冷凍再植實驗中,引入了急性血液稀釋技術(ANH),對比術中、術后動物血液循環動力學指標及全身狀態,報告如下:
1 材料和方法
1.1 一般資料
選擇成年實驗用比格犬16只,實驗動物由北京維通利華實驗動物技術有限責任公司提供。動物許可證號:SCXK(京)2011-0006。雌雄各半,體重(15±0.5)kg,隨機分為A、B兩組,對照組(A組)采用靜脈補充等量乳酸鈉林格氏液,實驗組(B組)采用急性血液稀釋技術。在解放軍軍事醫學科學院實驗室操作,實驗動物使用合格證號:SYXK-(軍)2012-0021。實驗過程中對動物處置方法符合《關于善待實驗動物的指導性意見》。
1.2 手術過程
術前40 min B組采犬靜脈血150 mL,同時輸注乳酸鈉林格氏液250 mL,A組不采血,直接輸注乳酸鈉林格氏液100 mL;術前10 min檢測A、B兩組血壓、心率、呼吸、血紅蛋白、紅細胞壓積。經口腔插管全身麻醉成功后,常規消毒鋪巾,自犬脛腓骨中遠1/3處離斷,將肢體遠端灌注后階梯式降溫至-196攝氏度,存放1 h后再階梯式復溫至常溫,行斷肢再植手術,A、B兩組手術操作相同,手術結束前30 min檢測A、B兩組血壓、心率、血紅蛋白、紅細胞壓積,心電圖(EKG),氧飽和度(SpO2),而后將B組術前所采自體血回輸;同時A組輸注乳酸鈉林格氏液150 mL,手術歷時約7 h,全部實驗組均由同一組手術人員執行,術后60 min復測上述指標(圖1)。

圖1 左上:實驗動物及血袋;(upper left),preoperative preparation(lower left),and post-operation blood transfusion(right)Fig.1 The experimental animal and blood bag
1.3 觀察指標
1.3.1 術前:術前10 min、檢測A、B兩組血壓、心率、呼吸、血紅蛋白、紅細胞壓積。
1.3.2 術中:手術結束前30 min,檢測A、B兩組血壓、心率、血紅蛋白、紅細胞壓積,心電圖(EKG),氧飽和度(SpO2)。
1.3.3 術后:術后60 min,檢測A、B兩組血壓、心率、呼吸、血紅蛋白、紅細胞壓積,同時觀察記錄A、B組動物術后蘇醒時間,抬頭時間,站立時間,術后首日進食量(實驗動物飼料克)、進水量(mL)。
1.4 統計學方法
表1 術前10 min監測指標(±s)Tab.1 Monitoring indicators at 10 min before operation(±s)
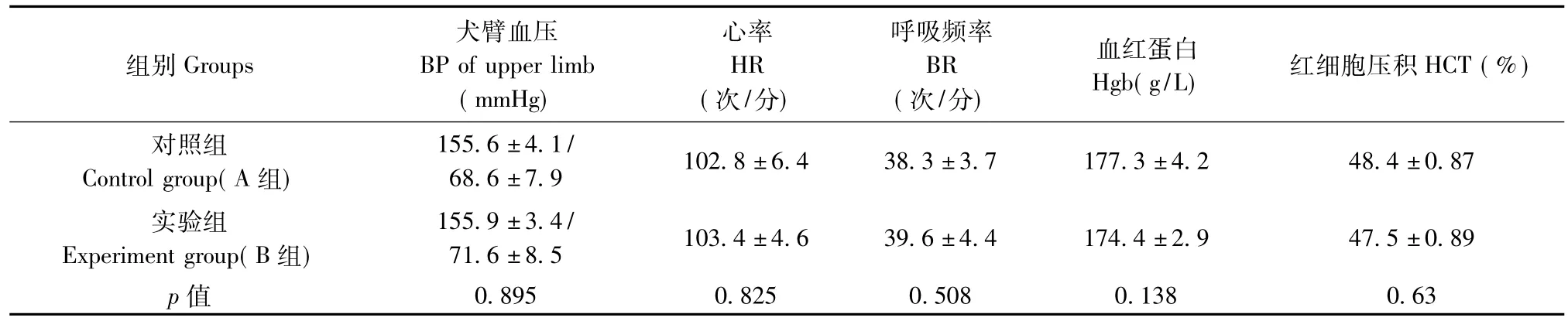
表1 術前10 min監測指標(±s)Tab.1 Monitoring indicators at 10 min before operation(±s)
注:A、B兩組血壓、心率、呼吸、血紅蛋白、紅細胞壓積p值均大于0.05,差異無顯著性,認為ANH技術對犬術前狀態無明顯影響。Note.There was no significant difference in BP,HR,BR,Hgb and HCT between the two groups(P>0.05).ANH had no obvious effect on the dog preoperative status.
組別Groups犬臂血壓BP of upper limb(mmHg)心率HR(次/分)呼吸頻率BR(次/分)血紅蛋白Hgb(g/L)紅細胞壓積HCT(%)對照組Control group(A組)155.6±4.1/68.6±7.9 102.8±6.4 38.3±3.7 177.3±4.2 48.4±0.87實驗組Experiment group(B組)155.9±3.4/71.6±8.5 103.4±4.6 39.6±4.4 174.4±2.9 47.5±0.89 p值0.895 0.825 0.508 0.138 0.63
表2 手術完成前30 min監測指標(±s)Tab.2 Monitoring indicators at 30 mins before the completion of operation(±s)
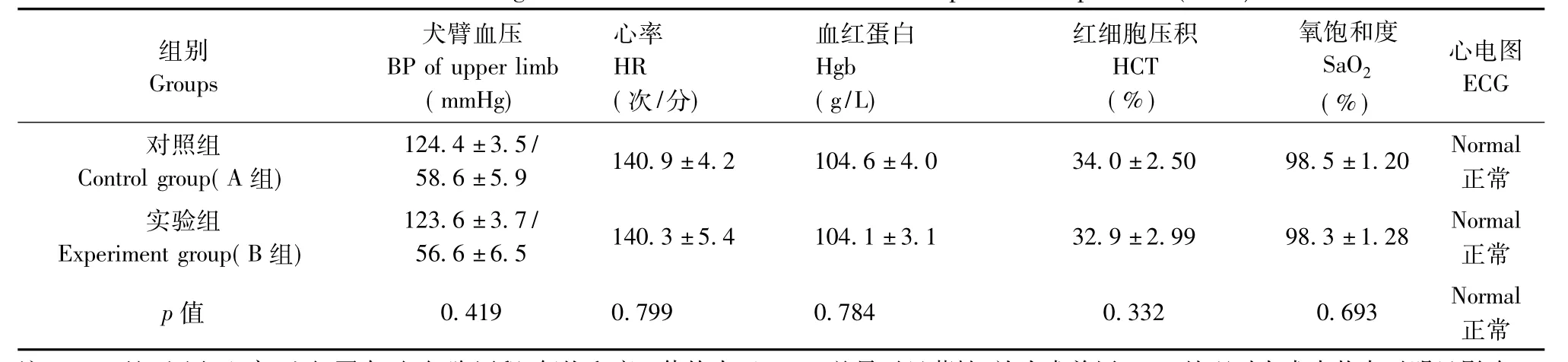
表2 手術完成前30 min監測指標(±s)Tab.2 Monitoring indicators at 30 mins before the completion of operation(±s)
注:A、B兩組血壓、心率、血紅蛋白、紅細胞壓積、氧飽和度p值均大于0.05,差異無顯著性,認為術前用ANH處理對犬術中狀態無明顯影響。Note.There was no significant difference in BP,HR,BR,Hgb,HCT and SaO2 between the two groups(P>0.05).ANH had no obvious effect on the dog during the operation.
組別 犬臂血壓 心率 血紅蛋白 紅細胞壓積 氧飽和度 心電圖GroupsBP of upper limbHRHgbHCTSaO2ECG(mmHg)(次/分)(g/L)(%)(%)對照組124.4±3.5/140.9±4.2 104.6±4.0 34.0±2.50 98.5±1.20 Normal Control group(A組)58.6±5.9 正常實驗組123.6±3.7/140.3±5.4 104.1±3.1 32.9±2.99 98.3±1.28 Normal Experiment group(B組)56.6±6.5 正常p值 0.419 0.799 0.784 0.332 0.693 Normal正常
表3 術后60 min監測指標(±s)Tab.3 Monitoring indicators at 60 min after the complation of operation(±s)

表3 術后60 min監測指標(±s)Tab.3 Monitoring indicators at 60 min after the complation of operation(±s)
注:A、B兩組血壓、呼吸、氧飽和度p值均大于0.05,差異無顯著性;兩組心率、血紅蛋白、紅細胞壓積p值均小于0.05,差異存在顯著性,認為應用ANH技術,血液回輸后實驗犬術后心率明顯降低,同時可明顯提高術后血紅蛋白及紅細胞壓積。Note.There was no significant difference in BP,HR and SaO2between two groups(P>0.05),but HR,Hgb,HCT in the experiment group were different from those in control group(P<0.05).It suggested that dogs in the experiment group had lower HR and higher Hgb and HCT than the control group after operation.
組別 犬臂血壓 心率 呼吸頻率 血紅蛋白 紅細胞壓積 氧飽和度GroupsBP of upper limbHRBRHgbHCTSaO2(mmHg)(次/分)(次/分)(g/L)(%)(%)對照組141.4±3.6/129.1±26.4 33.9±3.0 116.0±4.2 30.1±1.70 96.4±0.9 Control group(A組)73.6±8.9實驗組143.1±2.23/116.1±3.14 35.0±2.9 144.4±3.1 40.8±1.64 96.8±1.0 Experiment group(B組)74.6±9.5 p值0.261 0.000 0.467 0.000 0.000 0.456
表4 手術時間和術后動物狀態(±s)Tab.4 The conditions of during operation and post-operation(±s)
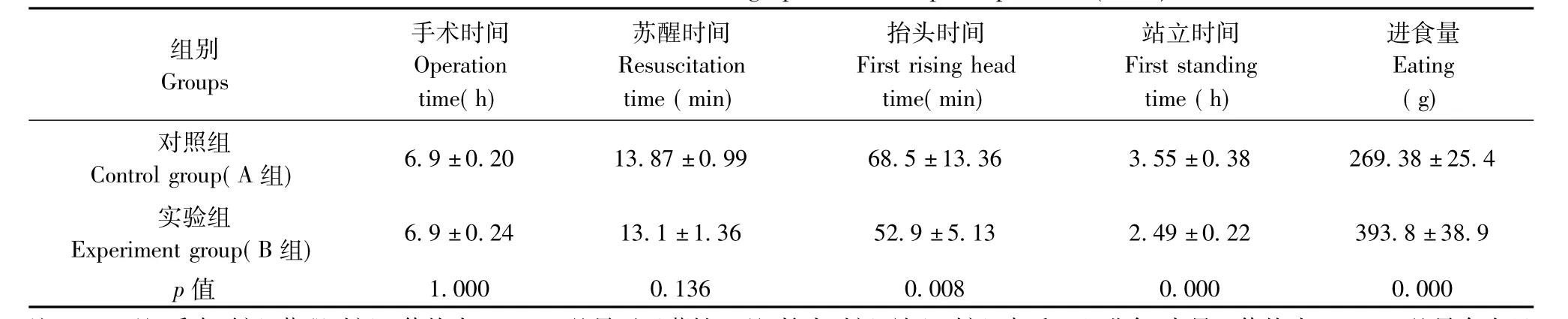
表4 手術時間和術后動物狀態(±s)Tab.4 The conditions of during operation and post-operation(±s)
注:A、B兩組手術時間、蘇醒時間p值均大于0.05,差異無顯著性;兩組抬頭時間、站立時間、術后24h進食、水量p值均小于0.05,差異存在顯著性,認為應用ANH技術,能夠明顯改善實驗犬的術后狀態,使其盡快抬頭、站立、進食水,但進水量較對照組減少。Note.There was no significant difference in operation time and resuscitation time between the two groups(P>0.05),but first rising head time,first standing time and eating and drinking intake in the experiment group were different from those in of the control group(P<0.05).It suggested that dogs in the experiment group restored earlier than the control group.
組別 手術時間 蘇醒時間 抬頭時間 站立時間 進食量GroupsOperationResuscitationFirst rising headFirst standingEating time(h)time(min)time(min)time(h)(g)對照組6.9±0.20 13.87±0.99 68.5±13.36 3.55±0.38 269.38±25.4 Control group(A組)實驗組6.9±0.24 13.1±1.36 52.9±5.13 2.49±0.22 393.8±38.9 Experiment group(B組)p值1.000 0.136 0.008 0.000 0.000
2 結果
2.1 術前
術前10 min(備血后)、檢測A、B兩組血壓、心率、呼吸、血紅蛋白、紅細胞壓積,各組數據應用SPSS17.0統計軟件處理,采用兩獨立樣本的t檢驗(表1)。
2.2 術中
兩組麻醉機設置相同的呼吸頻率、潮氣量及氧濃度,手術結束前30 min,檢測A、B兩組血壓、心率、血紅蛋白、紅細胞壓積,心電圖(EKG),氧飽和度(SpO2),各組數據應用SPSS17.0統計軟件處理,采用兩獨立樣本的t檢驗(表2)。
2.3 術后
手術結束前30 min將B組術前所采自體血回輸,同時A組輸注乳酸鈉林格氏液150 mL;術后實驗犬均順利拔管、蘇醒,術后60 min,檢測A、B兩組血壓、心率、呼吸、血紅蛋白、紅細胞壓積,同時觀察記錄A、B組動物手術時間、術后蘇醒時間,抬頭時間,站立時間,術后首日進食量(實驗動物飼料克)、進水量(mL)。各組數據應用SPSS 17.0統計軟件處理,采用兩獨立樣本的t檢驗(表3、4)。
由上述結果可見,急性血液稀釋技術可以有效降低術中實際出血,改善動物術后貧血,縮短動物復蘇時間,使動物快速恢復到術前狀態,進而保證實驗的順利進行,同時減輕了實驗動物的痛苦。
3 討論
一種創新技術、創新手術在進入臨床前必須進行大量的嚴格的活體動物實驗,而其中需要復雜手術操作的活體動物實驗失敗的主要原因除了手術操作失誤以外,很大一部分因素是因為手術時間長、創傷大、出血多,造成動物術中、術后休克死亡,所以輸血對需要復雜手術操作的活體動物實驗就顯得尤為重要[1-3]。但對動物輸血目前只有美國、澳大利亞等發達國家以中央血庫的形式建立了動物血庫,目的是治療寵物和拯救瀕危動物,而非動物實驗用血庫[4-7];國內因為成本太高目前尚無動物血庫,僅少量寵物醫院采用臨時同種異體輸血方式對救治的寵物進行輸血,但寵物品種繁多,血型也多種多樣,如犬的血型至少有8種,貓有6種,羊有9種,而牛的血型多達40種以上,且無統一的檢測標準,存在巨大的安全問題,更無法在動物實驗中廣泛應用[8-11]。
人類探索安全輸血經歷了長達400年的歷程,隨著對異體輸血弊端認識的深入,人們已逐漸接受并提倡自體輸血,并出現了術前自體采血貯存技術(preoperative active blood donation,PABD)、急性血液稀釋技術(acute normovolemic hemodilution)、術中及術后術區血液回收技術(intraoperative and postoperative blood salvage)等自體輸血技術。但目前術前自體采血貯存技術和術中及術后血液回收技術都需要專業的血液采集、儲存、凈化等設備,費用昂貴,難以普及。而對于難以實現異體輸血的動物實驗,急性血液稀釋技術就成為一條重要的解決方法。
急性血液稀釋技術(ANH)是1946年發明的術中自體輸血的一種方式,現已廣泛應用于臨床[12,17]。ANH一般是在麻醉后和手術主要步驟開始之前,短時間內快速抽取患者預定量的自體血液貯存于手術間,同時補充等效容量的晶體或膠體液,快速稀釋血液,有輸血指征或手術結束前再將采集的新鮮自體血回輸給患者[12,13,17]。其優點有:(1)ANH可使術中血液稀釋,降低在手術操作過程中循環中的紅細胞濃度,減少術中紅細胞流失,使手術中的實際出血量減少,以達到不輸異體血或少輸異體血的目的[13];(2)ANH是唯一提供新鮮自體血液的方法,血小板及凝血因子功能基本不受影響,紅細胞損失少;(3)自身輸血,無抗原性及過敏反應的風險,對術后免疫學檢查影響小[14,15,16]。
斷肢冷凍再植實驗手術創傷大,手術時間長,出血多,我們將ANH應用到此實驗中,研究結果顯示,ANH可以有效降低術中實際出血,糾正術后貧血,同時縮短動物術后抬頭、站立時間,改善術后動物全身狀態。
綜上所述,對于需要復雜手術操作的活體動物實驗,急性血液稀釋技術可以有效降低術中實際出血,改善動物術后貧血,縮短動物復蘇時間,使動物快速恢復到術前狀態,進而保證實驗的順利進行;同時ANH減輕了實驗動物的痛苦,符合動物實驗倫理學的要求,操作簡單,費用低廉,值得進一步推廣。
[1]Tremper KK.48thAnn Reference Course Lectures and Clin Update Program Am Soc Ansthesiologists[M].1997,7:113.
[2]Kl?vekorn WP,Pichlmaier H,Ott E,et al.Akute praeoperative Haemodilution eine Moeglichkeit zu autologen Bluttransfusion[J].Chirurg,1974,45:452-458.
[3]Matot I,Scheinin O,Jurim O,et al.Effectiveness of acute normovolemic hemodilution to minimize allogeneic blood transfusion in major liver resections[J].Anesthesiology,2002,97(4):974-800.
[4]Gross JB.Estimating allowable blood loss:corrected for dilution[J].Anesthesiology,1983,58:277-280.
[5]Estafanous FG,Mekhail N,Yared JP.Advantages limitations of hemodilution[J].Semin Thorac Surg,1994,6:87-89.
[6]Habler OP,Kleen MS,Podtschaske AH.et al.The dffect of acute normovolemic hemodilution on myocardial contractility in anesthetized dogs[J].Analg,1996;83(2):451-458.
[7]Leung JM,Weiskopf RB,Feiner J.et al.Electrocardiographic ST-segment change during acute severe isovolemic hemodilution in humans[J].Anesthesiology,2000,93(4):1004-1010.
[8]Weiskopf RB.Hemodilution and candles[J].Anesthesiology,2002,97(4):773-775.
[9]Van Der Linden P,Wathieu M,Gilbart E,et al.Cardiovascular effects of moderate normovolaemic haemodilution during enflurane-nitrous oxide anaesthesia in man [J].Acta Anaesthesiol Scand,1994,38:490-498.
[10]Ickx BE,Rigolet M,Van der Linden PJ.Cardiovascular and metabolic response to acute normovolemic anemia[J].Anesthesiology,2000,93:1001-1016.
[11]Jones,SB,Whitten,CW,Monk,TG.Influence of crystalloid and colloid replacement solutions on hemodynamic variables during acute normovolemic hemodilution[J].J Clin Anesth,2004,16(1):11-7.
[12]牛新環,田玉科,張咸偉,等.急性等容性血液稀釋與自體血回輸對病人血電解質和血漿蛋白的影響[J].臨床麻醉學雜志,2004,20(2):109-110.
[13]Stehling LC.A Report by the American Society of Anesthesiologists Task Force on Blood Component Therapy.PracticeGuidelines forBlood ComponentTherapy[J].Anesthesiology,1996,84:732-747.
[14]Miller RD.Coagulation and packed red cell transfusion[J].Anesth Analg,1995,80:215-216.
[15]Hobisch-Hagen P,Wirleitner B,Mair J,et al.Consequences of acute normovolaemic haemodilution on haemostasis during major orthopaedic surgery[J].Br J Anaesth,1999,82(4):505 -509.
[16]Bourke DL,Smith TC.Estimating allowable hemodilution[J].Anesthesiology,1974,41:609-612.
[17]效小莉,錢桂蘭,劉嵐.圍產期急性等容稀釋性自體輸血安全性研究[J].中國輸血雜志,2013,(1):63-64.
Acute normovolemic hemodilution in cryopreserved dog limb replantation
ZHU Ze-Xing1,ZHANG Shu-Ming1,ZHAO Yong-Jun2,FAN Kai-Bin3,QIAO Lin1
(1.Department of Orthopaedics,the Second Artillery General Hospital,BeiJing 100088,China;2.Department of Orthopaedics,Armed Police Medical School affiliated Hospital,Tianjin 300160;3.Department of Orthopaedics,Handan Central Hospital,Handan,Hebei 056001)
Objective To observe the contribution of acute normovolemic hemodilution(ANH)in experiment of cryopreserved dog limb replantation.Methods Sixteen healthy Beagle dogs(male:female=1:1)were divided into two groups.Dogs in the experiment group(Group B)
ANH in the limb replantation,and dogs in the control group(Group A)received the same amount of lactate Ringer’s solution intravenously during the surgical operation.We recorded and compared the hemodynamic indexes,HB,HCT,the resuscitation time,the first rising head time,the first standing time and the first eating and drinking time between the two groups.Results (1)During the operation,both PaO2and PCO2in the two groups were normal,as well as the breathing rate.The heart rate in the group B was lower than that in the group A.Before blood transfusion,there was no statistically significant difference in HB and HCT between the two groups,but after transfusion they were significantly higher in the group B than in the group A.(2)The resuscitation time,the first rising head time,the first standing time and the first eating and drinking time of the group B were all better than those in the group A.Conclusions In cryopreserved dog limb replantation experiments,acute normovolemic hemodilution is helpful to improve the general condition and facilitate the recovery of animals after limb replantation.
Dog;Limb replantation;Cryopreservation;Acute normovolemic hemodilution;Surgery
喬林(1971-),男,研究方向:創傷骨科。qiaolindoc@sohu.com。
R33
A
1671-7856(2015)04-0014-03
10.3969.j.issn.1671.7856.2015.004.003
軍隊“十二五”課題基金《冷凍肢體再植的研究》(編號:08G051)。
朱澤興(1981-),男,研究方向:創傷骨科、顯微外科。E-mail:zzxzxcvbn@163.com。
2015-02-15
猜你喜歡
小獼猴智力畫刊(2022年9期)2022-11-04 02:31:42
中學生數理化·中考版(2022年11期)2022-02-16 07:01:20
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
河北畫報(2020年10期)2020-11-26 07:20:50
小哥白尼(趣味科學)(2019年6期)2019-10-10 01:01:50
發明與創新(2016年38期)2016-08-22 03:02:52
太空探索(2016年5期)2016-07-12 15:17:55
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
西南軍醫(2014年5期)2014-04-25 07:42:48
中國中醫藥現代遠程教育(2014年13期)2014-03-01 04:26:36
