抗凝抗血小板藥物圍術期應用與起搏器植入術后囊袋血腫形成的關系研究
2011-06-13 01:03:02許偉源郭航遠
中國全科醫學 2011年35期
許偉源,郭航遠,彭 放
抗凝抗血小板藥物圍術期應用與起搏器植入術后囊袋血腫形成的關系研究
許偉源,郭航遠,彭 放
目的 研究圍術期應用抗凝及抗血小板藥物與起搏器植入術后囊袋血腫形成的關系。方法 回顧2007年1月—2010年1月在我院植入或更換起搏器患者的臨床資料,在不停用抗凝或抗血小板藥物的情況下,對其中血栓高危患者術后囊袋血腫發生情況進行分析。結果 共476例患者植入或更換起搏器,有14例出現圍術期囊袋血腫并發癥,發生率為2.9%,其中服用阿司匹林者6例,雙聯 (阿司匹林聯合氯吡格雷)抗血小板者5例,華法林者1例。進一步分析,雙聯抗血小板藥物者血腫發生率較未服用抗凝抗血小板藥物者、單用阿司匹林者為高 (發生率分別為17.9%,0.7%和4.3%,P<0.05)。所有囊袋血腫經適當處理后好轉出院。結論 起搏器植入術后囊袋血腫的發生率較低,阿司匹林聯合氯吡格雷明顯增加起搏器術后囊袋血腫的發生,手術經驗和恰當的術中操作有助于減少血腫的發生率。
心臟起搏器,人工;抗凝藥;血小板聚集抑制劑
起搏器作為治療心律失常的重要手段在臨床上已應用數十年,隨著起搏器功能日趨完善,其植入適應證也在不斷擴大,因此越來越多的患者接受了起搏器植入治療,其中不乏血栓事件的高危患者,特別是一些冠狀動脈藥物支架植入、心房纖顫、瓣膜置換術后等患者。圍術期繼續應用抗凝抗血小板藥物有可能增加起搏器植入術后發生囊袋血腫的風險,若停用上述藥物,又可能導致嚴重的血栓事件。圍術期能否應用這些藥物、如何應用,一直是臨床特征見表1。學術界爭論的焦點,但都缺乏明確的臨床證據。筆者回顧性分析了本院2007年1月—2010年1月行起搏器植入術患者的臨床資料,包括圍術期服用阿司匹林、氯吡格雷或華法林的患者,比較圍術期服用上述藥物對術后囊袋血腫發生率的影響。
1 資料與方法
1.1 一般資料 選擇2007年1月—2010年1月在我院行永久起搏器植入術,包括植入埋藏式心臟復律除顫器 (ICD)、心臟再同步治療 (CRT)、更換起搏器的患者共476人,其中男285例,女191例,平均年齡 (66.5±12.8)歲,患者均無嚴重肝、腎疾病及凝血功能障礙。患者的
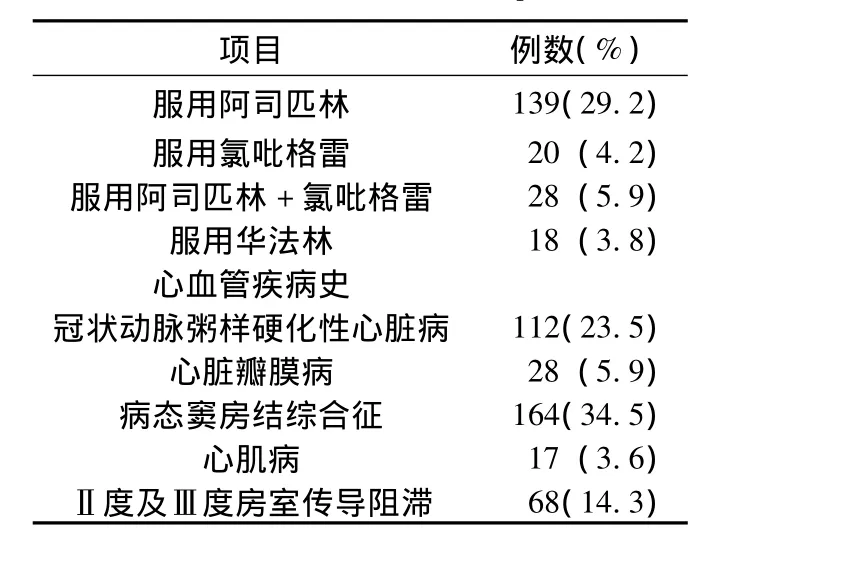
表1 患者的臨床特征Table 1 Clinical features of patients
1.2 植入方法 起搏器植入均采用鎖骨下靜脈途徑植入起搏器電極,術后囊袋部位沙袋壓迫12 h,起搏器植入側肢體制動24 h。所有患者在起搏器植入前沒有停用華法林、阿司匹林或雙聯 (阿司匹林聯合氯吡格雷)抗血小板藥物,拆線后第2天出院,患者術后1個月檢查起搏器囊袋及起搏器程控,期間有不適隨診。圍術期規定為術前5 d~術后1個月;囊袋部位出現>5 cm×5 cm瘀斑或血腫,則認為發生囊袋血腫形成。
1.3 統計學方法 應用SPSS 13.0軟件包進行分析,計數資料采用χ2檢驗,以P<0.05為差異有統計學意義。
2 結果
2.1 囊袋血腫發生情況 圍術期應用阿司匹林腸溶片者139例,氯吡格雷者20例,雙聯抗血小板者28例,華法林者18例,其中新植入起搏器者423例,更換起搏器者46例,起搏器升級者7例。共14例患者出現圍術期囊袋血腫并發癥,其中服用阿司匹林者6例,雙聯抗血小板藥物者5例,華法林者1例,未用抗凝抗血小板藥物者2例。服用不同藥物者比較,囊袋血腫發生率間差異有統計學意義 (χ2=28.56,P<0.05,見表2);兩兩比較,除服用華法林與阿司匹林、氯吡格雷,氯吡格雷與未用抗凝抗血小板藥物者比較差異無統計學意義外,余均有統計學意義(P<0.05);雙聯抗血小板藥物者血腫發生率較未服用抗凝抗血小板藥物者、單用阿司匹林者為高 (發生率分別為17.9%,0.7%和4.3%,P<0.05)。
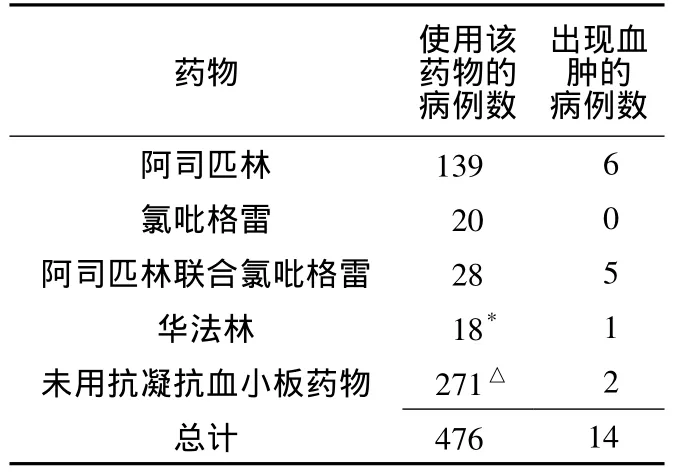
表2 各組囊袋血腫發生情況 (例)Table 2 Incidence of pocket hematoma of each group
2.2 囊袋血腫的嚴重程度及處理 2例通過延長局部沙袋壓迫時間,5例通過無菌注射器穿刺抽出積血,彈力繃帶加壓包扎,局部沙袋壓迫等治療后好轉;3例局部注射凝血酶,4例 (其中3例為雙聯抗血小板藥物患者)通過手術室重新打開囊袋,手術探查止血,清除血凝塊后再清創縫合后好轉。
3 討論
生理止血過程包括損傷后小血管收縮,血小板和血漿中的凝血系統激活,血小板黏附聚集形成松軟的止血栓以填塞傷口,纖維蛋白原轉變成不溶的纖維蛋白分子多聚體,并形成由血纖維與血小板構成的牢固止血栓,有效地制止出血[1]。阿司匹林通過抑制環氧化酶、血栓素A2的生成從而抑制血小板聚集;氯吡格雷可與血小板表面的ADP受體結合,抑制血小板膜糖蛋白Ⅱb/Ⅲa(GPⅡb/Ⅲa)活化進而抑制血小板的聚集[2-3];肝素通過抑制凝血酶原激酶的形成,增強抗凝血酶Ⅲ活性,抑制纖維蛋白原轉變為纖維蛋白,防止血小板的聚集和破壞[4]。與肝素相比,華法林并非特異性地抑制血小板功能,而是干擾維生素K依賴性凝血因子Ⅱ、Ⅶ、Ⅸ、Ⅹ的羧化使其無法活化而達到抗凝的目的[5]。這些藥物雖然作用機制不同,但均影響凝血過程,有增加術后出血可能。
由于起搏器植入患者中不乏血栓事件的高危患者,起搏器植入圍術期能否應用抗凝抗血小板藥物一直是學術界爭論的焦點,目前仍沒有明確在起搏器植入期間是否需要暫時停用抗凝抗血小板藥物,及停用多久。有研究建議使用華法林的患者在圍術期應用低分子肝素替代[6-7],以降低出血風險,但另有臨床數據表明用肝素替代療法有高達20%的出血風險,高于持續應用華法林的2%~4%的風險,提示肝素替代的方法并不能降低出血風險[8-9]。本研究表明服用華法林的患者囊袋血腫發生率與未用抗凝抗血小板藥物的患者相比,無顯著差異,與國外文獻報道一致[10-12]。
本研究顯示,服用阿司匹林的患者植入起搏器術后囊袋血腫的發生率較未服用抗凝抗血小板藥物者高,且雙聯抗血小板較單用阿司匹林或氯吡格雷進一步增加術后囊袋血腫的風險。隨著介入治療、藥物支架的廣泛開展和應用,常需要患者服用雙聯抗血小板藥物1年以上,以減少支架內血栓的形成[13]。一些學者建議對這些患者盡量延遲起搏器植入,避免在雙聯抗血小板期間手術,以期減少出血風險,但尚缺乏延遲起搏器植入帶來的益處與風險的比較,何者獲益更大的證據。
囊袋血腫除了應用抗凝抗血小板藥物的影響外,手術操作不當也是常見原因。術中傷及小動脈,解剖層次不分,損傷胸大肌筋膜,術中止血不徹底等均是術后囊袋血腫形成的常見原因。手術經驗和手法在避免此并發癥中具有重要意義,本院在穿刺鎖骨下靜脈成功留置導引鋼絲后,即開始制作起搏器囊袋,并用腎上腺素生理鹽水稀釋液沖洗囊袋,使小血管收縮,減少滲血,然后填塞無菌干紗布以使囊袋保持一定張力,待準備放入起搏器時,囊袋內已相對干燥無出血或滲血,出血機會減少;其次手術切口時解剖層次要清晰,避免損傷胸大肌筋膜,避免局部皮膚張力過大,影響切口愈合,在術中除了縫扎明顯出血點外,縫扎電極導線在鎖骨下靜脈穿出的皮下組織部位也很重要,一方面可達到固定電極導線的目的,另一方面消除了電極導線作為引流條將不能迅速閉合的靜脈滲血引流到囊袋內的可能。這可能是本院起搏器術后囊袋血腫的發生率(2.9%)較一些文獻報道低的原因[14]。
本研究提示起搏器植入術后囊袋血腫的發生率是比較低的,阿司匹林聯合氯吡格雷明顯增加起搏器術后囊袋血腫的發生,適當的圍術期管理有助于對出血風險和血腫形成的認識和評估,手術經驗和恰當的術中操作有助于減少血腫的發生率。本研究樣本量有限,不可避免會產生偏倚,有待于更多的臨床經驗和循證醫學證據的積累。
1 Furie B,Furie BC.Mechanisms of thrombus formation[J].N Engl J Med,2008,359(9):938-949.
2 Maree AO,Fitzgerald DJ.Disease variable platelet response to aspirin and clopidogrel in atherothrombotic disease [J].Circulation,2007,115(16):2196-2207.
3 Vane JR,Botting RM.The mechanism of action of aspirin [J].Thromb Res,2003,110(5-6):255-258.
4 Hirsh J,Warkentin TE,Shaughnessy SG,et al.Heparin and low - molecular- weight heparin:mechanisms of action,pharmacokinetics, dosing, monitoring, efficacy and safety [J].Chest,2001,119(1 Suppl):64S -94S.
5 Hirsh J,Dalen J,Anderson DR,et al.Oral anticoagulants:mechanisms of action,clinical effectiveness and optimal therapeutic range[J].Chest,2001,119(1 Suppl):8S -21S.
6 Hirsh J,Fuster V,Ansell J,et al.AHA/ACC foundation guide to warfarin therapy[J].J Am Coll Cardiol,2003,41(9):1633-1652.
7 Hirsh J, Anand SS,Halperin JL, et al.Guide to anticoagulant therapy:heparin,a statement for healthcare professionals[J].Circulation,2001,103(24):2994 -3018.
8 Tompkins C,Cheng A,Dalal D,et al.Dual antiplatelet therapy and heparin" bridging"significantly increase the risk of bleeding complications after pacemaker or implantable cardioverter-defibrillatordevice implantation[J].J Am Coll Cardiol,2010,55(21):2376-2382.
9 Jamula E,Douketis JD,Schulman S.Perioperative anticoagulation in patients having implantation of a cardiac pacemaker or defibrillator:a systematic review and practical management guide [J].J Thromb Haemost,2008,6(10):1615-1621.
10 Thal S,Moukabary T,Boyella R,et al.The relationship between warfarin,aspirin,and clopidogrel continuation in the peri-procedural period and the incidence of hematoma formation after device implantation[J].Pacing Clin Electrophysiol,2010,33(4):385-388.
11 Goldstein DJ,Losquadro W,Spotnitz HM.Outpatient pacemaker procedures in orally anticoagulated patients[J].Pacing Clin Electrophysiol,1998,21(9):1730 -1734.
12 al-Khadra AS.Implantation of pacemakers and implantable cardioverter defibrillators in orally anticoagulated patients[J].Pacing Clin Electrophysiol,2003,26(1 Pt 2):511-514.
13 Grines CL,Bonow RO,Casey DE,et al.Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents:a science advisory from the American Heart Association,American College of Cardiology,Society for Cardiovascular Angiography and Interventions,American College of Surgeons,and American Dental Association,with representation from the A-merican College of Physicians[J].J Am Coll Cardiol,2007,49(6):734 -739.
14 Chow V,Ranasinghe I,Lau J,et al.Peri-procedural anticoagulation and the incidence of haematoma formation after permanent pacemaker implantation in the elderly [J].Heart Lung Circ,2010,19(12):706 -712.
Relationship between Continuation of Anticoagulant or Antiplatelet Drugs during Peri-procedural Period and Incidence of Hematoma Formation after Device Implantation
XU Wei-yuan,GUO Hang-yuan,PENG Fang.Department of Cardiology,Shaoxing People's Hospital,Shaoxing 312000,China
ObjectiveTo investigate the relationship between anticoagulant or antiplatelet drugs continuation in the peri-procedural period and the incidence of hematoma formation after device implantation.Methods Retrospectively review the clinical information of the patients undergoing pacemaker implantation or replacement at our hospital from January 2007 to January 2010.Analyze the incidence of Hematoma formation after Device Implantation in the patients with high-risk of Thrombosis,under the condition of continuous use of anticoagulant or antiplatelet drugs in the peri-procedure period.ResultsAmong the 476 patients implanted permanent pacemaker(PPM),14 patients had Capsular Hematomas during Peri-operation period,accounting for 2.9%of the total patients,among which 6 took aspirin(ASA),1 was on warfarin and 5 were on dual-antiplatelet(DAPT)therapy.The Incidence of Hematoma Formation on dual-antiplatelet therapy increased Significantly(P <0.05).Pocket Hematoma was gradually absorbed by properly management.ConclusionThis study suggests that hematoma formation after PPM implantation is rare,even among those who are anticoagulated.Use of DAPT can imcrease the incidence of Hematoma formation.Surgical experience in the operation and proper technique can help reduce the incidence of hematoma.
Pacemaker,artificial;Anticoagulants;Platelet aggregation inhibitors
R 654.29
A
1007-9572(2011)12-4106-03
312000浙江省紹興市人民醫院心內科
2011-05-20;
2011-11-10)
(本文編輯:鹿飛飛)